On my first day in Nursing Fundamentals Clinical, my instructor shared a typical schedule to follow when we’re on the floor and the expected flow of the day. My instructor explained how the nurse has to keep organized to ensure the nurse properly assesses each patient, gives medications on time, takes vital signs as needed, provides education, addresses orders, and documents care. One of my classmates asked how a nurse keeps track of everything, and my instructor responded, “Oh, I use my brain.”
My classmates looked at one another, perplexed. I wondered, “How will I hold all that information and remember everything I have to do in my brain?!?” Only later, with some further explanation from my instructor, did we realize the “brain” on which she was relying to stay organized is a document and not an organ in her body.
A nurse’s “brain” is a document that helps a nurse stay organized and allows the nurse to take notes for shift handoffs, doctor’s reports, or assessments. A nurse can also use a brain to track: treatment or surgery, when to give medications or perform additional tasks, inputs, and outputs, progression of care, or the completion of orders. Of course, the nurse documents care within a patient’s chart. However, a nurse’s “brain” serves as a mini notepad or planner for the nurse between charting.
In nursing school, I was exposed to and used various types of brains. There are numerous templates for brains available, and some are even free. During nursing school, I liked trying the brains offered by nursing.com. (With a subscription, the website provides a brainsheet database of 33 different brains, some focused on specialties like ICU, Peds, or L&D). Often, units in hospitals print specific brains for staff to use. However, it is the nurse’s preference that determines the brain a nurse uses. For instance, my preceptor never uses the unit’s pre-printed brains and writes out her brain every time she shifts. While nurses are not required to use a brain, I don’t believe I’ve ever met a nurse who doesn’t use one.
After attempting to use multiple brains, I decided to design my own. Some brains don’t have enough space, are not organized the way I want, or do not capture the information I need. As a new grad nurse, I find it difficult to track the completion of required charting or documentation unless I note it in my brain. No generic brain template is going to capture the documentation unique to my unit.
As I imagined what I wanted to include in the brain I was designing for myself, I read the book “The Checklist Manifesto: How to Get Things Right” by Atul Gawande. My husband received it as a gift, and he recommended the book to me. He thought it would interest me since the author was a surgeon exploring ways to make surgeries safer. The author worked with the World Health Organization (WHO) to develop a checklist to use for surgeries, to prevent errors (and ultimately, injuries or deaths due to preventable mistakes). It was a quick and fascinating read. He explored how other industries such as construction or airlines use checklists. As in surgery, errors in those industries can be fatal. At its worst, errors in construction or flying planes can be catastrophic and result in mass casualties. Yet, such errors are rare compared to mistakes in surgery. The book discusses how he and others developed a worldwide surgical checklist for WHO and what resulted. The author also shares when checklists are inappropriate and offers tips on developing them, even down to what font one should use. I enjoyed reading the book – it was a nice break from studying or reviewing nursing-related topics, yet I felt it was helpful to me as a nurse.
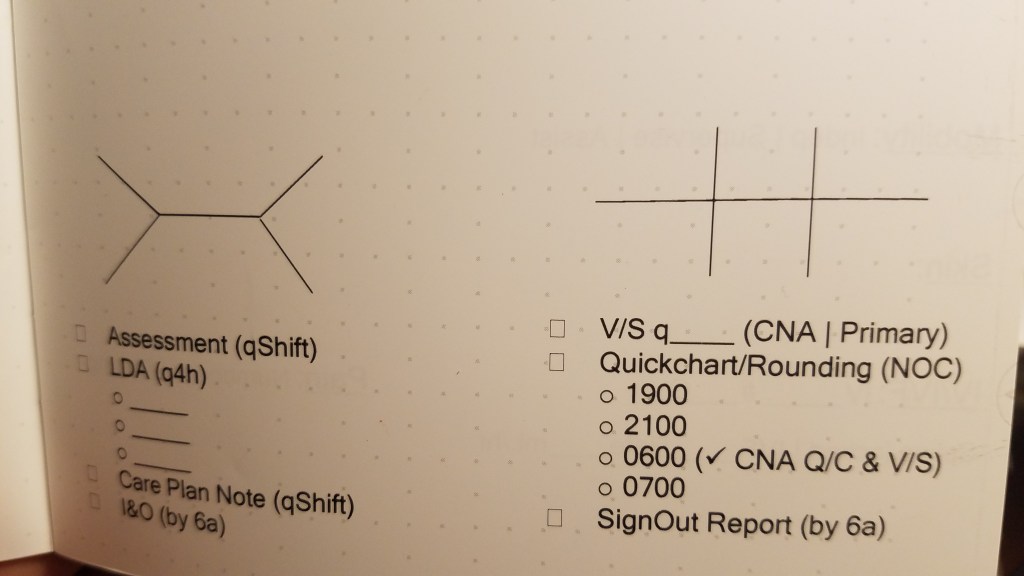
Considering what I learned from Atul Gawande, I placed a documentation checklist onto my brain template. Since I’ve set the documentation checklist in my brain, I’ve been more efficient in my charting. I can ensure I’ve completed the charting documentation for each patient without spending extra time combing through various sections of a patient’s chart to verify completion multiple times. My preceptor does not have to stay over later to complete missing documentation for our patients as she did earlier during my orientation and training. My checklist lets me know what I’ve done and what’s still missing during my shift. I know I’ve become more proficient at time management since starting orientation, but having the checklist helps me keep organized and manage my time. Plus, as a checklist gal, it feels satisfying when I cross off all the boxes in my checklist by the end of the shift.
Are there checklists you use day to day that help you in your personal life or your work? Or, are there brains you’ve used that you like? I’d love to hear and learn what works for others!

