Tag Archives: newgradnurse
Motivating Music
I have faced tough days as a student, mom, or nurse…Beyond prayer, music helps restore me and surrender my circumstances to God. What restores you? What do you do to bring peace or rebuild your confidence when you face uncertainty, have no control, or have had a rough day?
St. Augustine said, “Those who sing pray twice.” I love to sing, and music helps inspire me. Personally, songs from church help bring me peace. Below is the link to my Spotify playlist of songs that I listen to or sing to motivate me on tough days. May it inspire or encourage you.
Good luck on your journey!

What Nursing School Did Not Teach Me About Nursing, Part 3: Physical Endurance & Self-Defense
Nursing can be very physically demanding – many patients require assistance turning, lifting, or moving body parts or equipment. I attended a safe-patient handling workshop offered by Daniel Tiano, a physical therapist whose goal is to “enable healthcare workers to fulfill their vocation without being held back by pain and injuries.” He compared nurses to endurance athletes, constantly lifting, turning, pushing, and pulling hundreds of pounds over a 12-hour shift. While I work primarily with neonates now that I’m a NICU nurse, I can still get floated to pediatric or post-partum wards and handle heavy patients. Pediatric patients are not always light, easy-to-handle patients. I’ve cared for adolescents over 80 kg and adults (18-25 years old) in pediatric units.

I must handle my patients carefully to avoid ergonomic injuries, even with babies. [Tips: Raise and lower beds or cribs to prevent back strain! Get assistance when lifting patients, and use lifting tools!] I know from experience that I can hurt more than just my back when caring for babies. As a new mom, I developed tendonitis because I held my newborn with my wrists bent. My baby wasn’t heavy to carry, but I still injured myself. My tendonitis pain went away after treatment and physical therapy. I’m more conscious now and deliberate about holding babies with my wrists straight!
Aside from modifying my behaviors to make sure I don’t cause myself injury, I have to be alert to other people’s behaviors. Patients (or their families) can have behavioral issues and be violent. As a nurse, I have to be careful that certain patients do not harm my co-workers or myself. Unfortunately, one of my teenage patients attacked her sitter/nursing assistant during one of my recent shifts. A nurse must continually assess their patient and environment to keep not only their patients safe but themselves safe, too.
Some patients (or their visitors) have mental health or drug use issues that make them unstable. Other patients may have temporary delirium due to infection or illness, causing verbally or physically abusive behavior that they usually would not have. I have cared for patients that have tried to hit, kick, or bite me or have yelled, cursed at me, and called me names. This danger doesn’t exist only in adult units. My NICU colleague had a teenage patient throw a monitor at her when she floated to the Pediatric unit. Honestly, I have more physical and personal safety considerations each day in my nursing job than in my previous career. I think that says a lot considering I was a certified Hazardous Waste Operator (HAZWOP) who periodically cleaned up hazardous material spills while I was an engineer!
Anyone working in hospitality or customer service is probably used to dealing with all kinds of people. My former preceptor used to be a restaurant server, and she said it helped prepare her for dealing with all types of patients in nursing. However, nursing is very different from what I was used to in my prior career. I never felt unsafe or in danger of other people when I was at work. I worked in a secured facility for over 18 years – people from the street couldn’t walk in, and we didn’t serve the public at my site.
In contrast, when you work in a hospital, you see all kinds of people, and often, people are emotional, in unresolved suffering and pain, or the most unstable they have ever been. It’s a ripe environment for people to lash out, potentially violently. Healthcare workers encounter violent behavior so often that facilities often require their employees to get certification in Management of Assaultive Behavior (MAB). As a NICU nurse, I haven’t encountered violent parents (hopefully, this NEVER happens). Still, I have observed emotional and angry parents with whom I must be careful and anticipate volatile behavior.
Bedside nursing is a physically demanding job. A nurse should exercise, eat energizing foods, and get enough rest to stay healthy and physically well. That applies to ANYONE. However, a nurse must also act like an endurance athlete and self-defense master. Aside from the typical actions to stay physically well or safe, nurses must be aware of body mechanics and constantly read behavioral cues from others. Thankfully, I’ve been safe and injury-free so far, but I’m still trying to figure out how to be more healthy, so I have the stamina and longevity to be a bedside nurse. I’m on a journey and will continue to share. Stay tuned for the next part of my novice nurse series, where I discuss handling my emotions as a new nurse.
What Nursing School Did Not Teach Me About Nursing, Part 2: Mentality and Mindset Challenges as a Novice Nurse
Welcome to Part 2 from a series of posts about what I learned as a new nurse and the demands of nursing.
It took a while for me to transition into nursing and adjust to my newfound career and job expectations. After working over eighteen years with the same company in a consumer products/manufacturing setting, I grew accustomed to a certain rhythm in my job as an engineer/scientist. I was a salaried employee in my previous career as an engineer and never needed to clock in or out. Some days could be stressful when I was an engineer, but mainly, I could set my day-to-day schedule. I didn’t have a required shift to start by six or seven each morning. I would have project deadlines to meet, but they didn’t necessarily dictate what I did every hour of each workday. I could go to the bathroom when I pleased or schedule my lunch to eat with friends. I had a lunch squad. If I was behind with my schedule, I could stay late. When I wasn’t periodically supporting shift work in the manufacturing plant, I started my days mostly between 8a and 9a and ended around 6:30p – 8p. Each workday as an engineer, I did not have to consider getting my work assignments from a prior shift, passing work along, getting and giving shift reports, nor did I need someone to take over my work during my bathroom or meal breaks.
I work in a hospital now, so my shifts as a nurse are dictated each day. Sometimes, there’s no time for me to pee, drink, or eat as a nurse. I eventually get to do these things, but not necessarily when I want. Hourly tasks (assessments, med passes, labs, and patient ADLs) dictate each workday. My patients and their needs and orders direct my priorities for each day. I have no lunch squad. I can’t go on meal breaks with my co-workers because they need to cover my patients when I go on break. Sometimes, the charge nurse makes me go on my snack and meal breaks when I am not ready to ensure proper coverage. If I think things are a little slow or I have some downtime, that’s when admission or some unexpected event likely occurs. (This is why you never use the “Q” word – “quiet” – to describe the environment or shift around nurses – you jinx them into having a chaotic shift later).
I’ve learned it’s better to accomplish tasks early rather than on-time because one emergency or tricky issue can cause a delay to an entire planned schedule that was once “on time.” For example, when I was in Med-Surge, I had to do unscheduled sacral wound dressing changes for an incontinent, primarily immobile, continuously stooling patient. Each time I’d get help to turn and lift the patient, clean them, replace their diaper and linens, and do the dressing change, the patient would soil themselves and their new dressing. These kinds of time-consuming, unplanned activities aren’t limited to adult patients. More recently, when I was floating to our Pediatric ward, an ostomy bag for a hyperactive non-compliant preschool patient kept leaking and needed continual replacement. The patient would purposely peel off their ostomy bag and then resist having it changed. Even though the patient was a preschooler, one person needed to help hold down the patient and keep the patient still to allow another person to replace the ostomy bag. Such unplanned activities take time and can cause delays in other scheduled tasks. I was used to addressing shifting priorities and non-compliances as an engineer, but I never had hourly assignments that could jeopardize people’s health if completed late or improperly.

It was hard for me to account for unexpected, unscheduled tasks as a new grad nurse. It can still be frustrating, but I feel I’m not as flustered, and it doesn’t have to thwart the rest of my day. I have learned to do things as early as possible to leave room for the unexpected. My last NICU preceptor also encouraged me to accomplish tasks as soon as possible to be available to help other nurses. Thankfully, nurses in my department jump in and help one another. However, my preceptor warned they may not be as willing to help me if I’m always busy and unable to help them when they need assistance. As I shared, some activities require coordination of availabilities and assistance from other nurses or nursing attendants. I want to be a team player that others can count on for help. Accomplishing tasks early not only makes my life easier, preparing for the unexpected, but it also allows me to help others with their patients or tasks. However, even when I am able and want to accomplish tasks before they are due, I can’t always do this. For instance, I must still ensure meds are given in an appropriate timeframe and not too early to avoid overdosing patients.
Critical thinking and mental alertness cannot be lax as a nurse. (This is also how I justify my caffeine intake). At best, a nurse’s mistakes may cause inconvenience; at worst, permanent injury or death. Any mistake I made as a process engineer could cost hundreds of thousands of dollars, but it would never cause bodily harm or death. There was a lot of oversight, approvals, and quality control with my work as an engineer. I feel like there are fewer checks and balances for nurses for the tasks they complete.
A nurse performs activities based on orders and nursing judgment. There is no constant oversight or approval process when a nurse administers many medications or completes orders. In contrast to process engineering mistakes, a medication error can kill. Not reporting critical labs or assessment findings can cause delays in treatment or interventions. I can’t consult with a weekly project team if I’m behind on my nursing tasks. I have to figure out who to ask for help to catch up with my work or quickly judge if it’s acceptable to be late, reschedule a task, or if I need to escalate issues. Aside from impacting patient care, nursing mistakes and errors can threaten nursing licenses. When I made mistakes as an engineer, I may have received criticism and a poor performance rating, but I never worried that I’d lose my ability to work as an engineer.
Given the pressure and expectations of nursing, my anxiety levels are higher than when I was an engineer or scientist. Some stress is healthy and helps keep my patients and me safe by forcing me to focus, ask for help, or take time with unfamiliar tasks or medications. However, until I became a nurse, I never realized how common it was for nurses to have or develop hypertension, anxiety, or depression. I’ve heeded the warnings of veteran nurses who advised me not to take overtime if I don’t need it, lest I end up with hypertension, like them.
I did not switch careers only to develop medical issues from my job. It’s one thing to manage high blood pressure, generalized anxiety disorder, post-traumatic stress disorder, or major depressive disorder, but it’s another to develop these conditions because of one’s job. Nurses need healthy coping mechanisms, as stated in my last post. I respect that sometimes it’s not enough to have healthy coping mechanisms or rely on comfort wisdom; various conditions require medication. However, Kelsey Rowell, RN Career Coach and founder of @wholelifenurse shared recently on her Instagram, “If your nursing job is requiring you to go on or increase your medication to support your mental health, that is your sign to find a new job, take a break, or do something else.” I wholeheartedly agree with her statement. Since I’ve switched to NICU nursing, my anxiety levels are lower than when I was a Float nurse for adults. Part of that may be due to having more experience or not working the night shift for the moment, but I think my decreased stress is also because NICU nursing is a better fit for me. There are so many opportunities within nursing that if a particular job is causing medical or mental health issues, try changing your nursing job!
What’s also relieved some of the new grad anxiety and pressure is recognizing that nursing is a practice. With more time and experience, I can improve my nursing practice. With more exposure to various units or patients, I learn what I like or dislike about specific nursing roles and can set my boundaries and determine my career goals. With more experience, certain medications or typical treatments will become more familiar. I will more easily recognize the signs or symptoms of conditions I regularly encounter. I can determine which skills are essential to master for various units or roles. (Tip: time management is a critical skill, no matter where you work as a nurse)
I have accepted that I’m imperfect and will make mistakes. Even veteran nurses make mistakes. When making mistakes, it’s essential to be transparent to a charge nurse or provider to correct errors or get help and alignment to move forward. Mistakes can serve as lessons. I’ve made mistakes in my engineering and nursing career that I know I will not make again because I never want to feel as compromised or ashamed as when I made the mistakes.
I want to prevent making mistakes that injure or permanently damage patients. One of my NICU preceptors said to accept that I will make mistakes but to spend time making sure I don’t make medication errors. If I spend more time evaluating an unfamiliar medication, dosage, or route, I accept that I will appear slow because of my uncertainty. I will ask for help or clarification. I will move more slowly and risk falling behind on my tasks rather than harmfully administering medication.
ANY new job or career produces increased stress and mental challenges. Some level of discomfort is healthy and helps us to learn and grow. It takes time to learn the protocols or processes of a new organization or unit. No one is perfect, and we all make mistakes. Sometimes, you understand how to be more efficient or effective by making mistakes or witnessing them. It takes time to learn who to ask for help, what requires escalation, and the chain of command. Over time, we know the methods of communication our co-workers, bosses, or patients/clients prefer. Skills cannot improve until you’ve practiced and done them many times. Understanding all this and having the mindset that I’m still learning (“I’m developing, not deficient!“) has helped relieve some of my new grad/novice nurse anxiety.
I hope this post gave some insight into the mental challenges of nursing and the mindset one has to have to thrive as a novice nurse. If you have any advice on how to handle the pressures of nursing or the mental challenges, please share! Thanks for reading! My next posts in this novice nurse series will discuss how I address the physical and emotional challenges of being a nurse.
Caffeine + Viagra






Why I Cried At Work
I spent last Friday morning at work crying. I was in my new job at my new hospital and in training. The training I took Friday morning was a mandatory two-hour computer-based session about the Commercial Sexual Exploitation of Children or CSEC. I cried with the testimonials and the trauma described by survivors and experts in the field. I felt a combination of rage and helplessness while I watched and listened to the videos. Luckily, I was in an area where no one else was sitting around me, so I felt I could express my grief and despair without too much concern.
I think this is part of what scares me about being a pediatric nurse. I worry if I can emotionally regulate myself when working with abused or neglected children. I also wonder and hope I can recognize and report abuse should I ever encounter an abuse victim. As difficult as it was, I appreciated completing the training and felt it was valuable. As a nurse, I am a mandatory reporter and must report child abuse when I suspect it. However, I think the general population should also take the introductory training about the Commercial Sexual Exploitation of Children to increase awareness, recognize and reduce risks, and maybe correct misconceptions about victims.
It is unlikely that the public would voluntarily take a two-hour training about the Sexual Exploitation of Children. Despite this, I hope to educate my readers and others who come across my blog or social media posts, because I think it’s important and is something I can easily do to help victims of CSEC. Some of the things I learned from the training are found below:



I can cry and grieve for these children, but I also want to take action. Let me know if you learned anything new from this post or if you found it helpful. I’m also curious to learn and hear from others about ways they support victims of the commercial sexual exploitation of children.
Major Update: I Quit My Job!
I have not posted in a while because I have been busy with some life changes. I recently resigned from my new grad RN job and accepted an offer to work at another hospital. What could have possibly taken me away from my #1 choice hospital and my highly pursued new grad program? A spot in my dream unit, the NICU!
It was tough for me to leave my program since I felt like the people were supportive overall. I truly appreciated the environment, community, and staff. I was learning a lot and growing as a nurse. However, my experience as a new grad RN working in the Float pool with adult patients also affirmed that my ultimate goal is to work with babies in a NICU.
My hospital has a NICU, which was a big reason I applied to their new grad program – I had hopes to move into their NICU eventually, especially after having a NICU preceptorship during nursing school. However, after working as a resident, I learned that the NICU at the hospital where I was employed does not accept inexperienced NICU nurses. The NICU manager recommended I apply to an L&D fellowship after my Float Pool residency, and maybe I could transfer to the NICU afterward. That would mean the earliest I could go to our NICU would be 2023, and that’s with the caveat that I would get accepted into a competitive year-long L&D fellowship. I would be competing with other nurses whose ultimate goal is to be an L&D nurse and other more experienced nurses previously rejected from the L&D fellowship.
After learning all this, I had the opportunity to interview during a mass hiring event for another hospital. The hospital already had my application from earlier in the year, one of the 70+ positions I applied to before starting my new grad program. I shared I only wanted NICU positions – there was no other reason I’d leave my new grad program since it was a great program in a good hospital. I interviewed with the NICU manager at the new hospital via MS Teams in between scheduled night shifts. At the end of the interview, she shared she’d like to hire me. I gave my job three weeks’ notice once I passed the background check and received a target start date. I started orientation for my nightshift NICU position at the new hospital on Oct. 1, last Friday.
I know it’s customary to give two weeks’ notice, but I felt obligated to give my old hospital three weeks. I ended up working four more shifts than if I had only given two weeks’ notice. During those four shifts, I had the most brutal shift I’ve had since coming off preceptorship and working solo. If I had left sooner, I could have saved myself from experiencing the most horrendous shift I’ve had so far. Luckily, my last shift was smooth and helped build my confidence after feeling torn down and broken from the week before – I met my patient’s needs promptly, charted everything on time, gave good shift reports, and my patients had no incidents. At my last job, I ended on a good note and had valuable learning experiences. My horrible shift in the week leading to my final shift taught me that when I’m overwhelmed, not only should I delegate, I should escalate to the charge nurse or nurse leaders. I will remember how awful my experience was on that shift to remind me in my nursing practice: “When Overwhelmed, Delegate + Escalate!”
I will remember this lesson as I start my new job. I am excited to have the opportunity to be in a NICU again. The children’s hospital where I precepted during nursing school opened its new grad program about a month after starting my previous job. Various cohort-mates encouraged me to apply, but I decided I needed to give my program and hospital a fair chance. I passed the opportunity to apply to the children’s hospital NICU new grad program before learning that my hospital would not hire me into their NICU for at least two more years. I don’t regret not applying to that NICU program because I’m grateful for my experience and feel more confident as a nurse because of what I’ve learned working with adults. I gave my program a chance and put forth my best effort, and concluded that I wasn’t willing to wait years to reach my goal to be a NICU nurse.
The earnest pursuit of career goals is somewhat new to me. For years, I didn’t know what I wanted. I knew that I was comfortable but not necessarily excited or passionate about my previous career as an engineer/scientist. During performance reviews, I would dread when my manager would ask what 5-year plan was because I wasn’t inspired by what was around me. I didn’t want my manager’s job, and other than becoming more skilled, building my expertise, and gaining more leadership experience, I wasn’t sure what else to say. Now, it’s nice to have a goal (dayshift NICU nurse) and work towards it.
It’s still a little terrifying:
“What if I don’t like it?”
“What if the staff is mean at the new hospital?”
“What if it’s not what I thought?”
“What if I’m not good at it?”
“What if I can’t handle the long commute?”
“What if I can’t last long enough on nightshift to make it to dayshift?”
Sometimes, you don’t know if you’re going to like something or will be able to handle it until you give it a try. I also have to be open to the possibility of failure or making mistakes with this new job – it’s those moments where real growth occurs, however. That’s how I became a better engineer or scientist. I made a mistake and remembered not to do it again. It’s like doing something wrong a couple of times before you figure out how to do it right, or in the most efficient way.
I think a terrifying part of being a novice nurse is mistakes in healthcare can have a profound and permanent impact on a patient and patient’s family. If I made a mistake as an engineer or scientist, many processes and people were in place that ensured no one would get hurt or injured. Delays or mistakes I made may cost hundreds of thousands of dollars, but they would never hurt someone. As a nurse, I no longer have that sense of security or protection. It’s anxiety-provoking. I’ve met many nurses with high blood pressure, anxiety, or depression due to the stresses of this profession. I don’t want to develop health issues because of my chosen career. I went into this profession to help people, so I try focusing on how I can help or improve care vs. contemplating the many ways I can injure someone or how someone may injure me (a genuine consideration with adult patients).
I’m still a recent grad with less than a year of acute care experience and still developing. Fortunately, my employer views me as a new grad and is willing to train me as a NICU nurse. I consider my new position as an opportunity to learn, grow, and be a better nurse. I’m going to try to focus on that and becoming the best NICU nurse I can be. Wish me luck!
Persistence with the Night Shift
I’m still trying to manage my life working the night shift while parenting a young child. While I wish I could engage more with my daughter, I’m grateful that she and my husband are close because of their time together without me. I wish I could give my husband more breaks from caring for our daughter solo. Unfortunately, I can’t participate in family activities like back-to-school nights or family dinners when I work. Truthfully, even when I do NOT work, I’m still exhausted from working night shifts; I can’t participate as much as I want with family activities, even on days off.
It’s a lot of effort for me to focus and maintain my clarity with sleep deprivation. When I started the night shift, I had difficulty sleeping during the day between my shifts and trouble staying alert during my shifts. I’m three months into working nights (7p-7:30a), and I can sleep about 5 hours between night shifts compared to the 3 or 4 I would get before. I am also more alert and have more stamina to last me throughout my shifts compared to three months ago. However, I now have difficulty sleeping at night on my nights off. (It was 2:30 on Monday morning when I started to write this blog post because I couldn’t sleep and wasn’t tired).

Here is how my day(s) off went after my last shift Friday night:
8:30 a – Come home from work Saturday morning, still stressed after a rough night shift – the third of three-in-a-row.
11 a – After showering, eating, and replaying my night in my head, I finally fall asleep – and miss out on my family’s Saturday brunch outing spontaneously scheduled with a friend that morning.
3:30 p – I wake up later than my 1p target. I feel too tired and groggy to join my husband and daughter for their afternoon pool-time.
7ish p – We have dinner delivered because I’m too tired to help prepare anything.
10 p – Husband wakes me on the couch since I fell asleep somehow. He convinces me to move to our bedroom.
2:30 a – Wake up and have trouble going back to sleep.
4:00 a – Take melatonin, hoping it will help me sleep
6:07a – The time on my clock that I remember seeing before falling asleep
7:35 a – The time I woke up when my daughter turned on all our lights and insisted on noisily searching our room for her lost unicorn.
My husband and I spent the rest of my second day off of work taking our daughter to gymnastics, having family brunch, going to church, and visiting a family friend in the afternoon and again for dinner. I briefly fell asleep sometime in the afternoon after reading with my daughter in her bedroom – before my husband woke me so we could go for the afternoon visit with a family friend. I try to enjoy days off with my family but often feel like a zombie days after I work.
When I work, I’m unable to attain the recommended 7-8 hours of sleep. I don’t think I’ve made up for the sleep debt I’ve incurred and am unsure when, if, or how I’ll make up for it. My sleep schedule is entirely abnormal, and I’m often tired. I schedule myself to sleep during certain times, but my body does not comply. I’ll fall asleep during the day between shifts hoping to sleep 6-7 hours but will often wake up after 4-5 hours. I have blackout curtains, use earplugs, play beach waves as ambient noise, spray lavender mist on my pillows and bedding, and wear a travel eye mask to help me sleep.

I don’t have television in my bedroom, and I take all phones out of the room when I sleep. I sleep for longer durations when I eat before going to bed in the morning, take melatonin, and supplement with tart cherry concentrate (which helps regulate melatonin levels). I set my alarm as late as possible before work and try not to look at my clock or phone until that alarm has gone off, even if I am awake and lying in bed for hours. I meditate or pray in bed to relax and attempt to fall asleep again if I wake up before the alarm activates. To stay awake while working, I drink caffeine but avoid it after 2a during my shifts and on days when I’m not working.
I’m not fond of the idea of having to medicate my body to either sleep or stay alert. In reality, though, I live in a caffeinated culture. Coffee and tea helped me survive nursing school. They also helped me in my first job as a nurse working swabbing shifts before 5:30a. Many people I know consume caffeine daily to be alert or as part of their morning ritual, and they are not nurses, nor do they work night shifts. Maybe I should accept that caffeine (and melatonin) are part of my weekly routine as a night shift nurse.
To try weaning off some of the caffeine, I’ve tried replacing some of my coffee intake with cacao. It has helped me during the early morning hours at work (when I think it’s too late to consume more caffeine), keeping me up without giving me jitters or hand tremors. My nursing school best friend turned me onto a brand, Crio Bru. According to Crio Bru:
“Brewed cacao is 99.9% caffeine free, but contains theobromine, a naturally occurring stimulant found in cacao that can be longer lasting, milder, and more pleasant than caffeine.”
-Crio Bru (https://criobru.com/pages/crio-bru-brewed-cacao)
It’s roasted cacao nibs that brew just like coffee, but there’s no caffeine. I like to make Crio Bru drink in a french press and keep it sugar-free.

I’ve also discovered a sugar-free cacao powder by ChocoVivo that doesn’t require a french press to prepare (https://chocovivo.com/collections/cacao/products/100-cacao-full-spectrum-cacao-powder). The hot chocolate from ChocoVivo has a thicker consistency since the cacao is not getting filtered out and is reminiscent of the hot chocolate I had with churros in Spain. It’s like drinking a dark chocolate bar. I sometimes like to add a little cinnamon to it.
I’ve been trying various techniques and methods to sleep or stay awake, stubbornly trying to make night shift work, because I eventually want to move out of my current position working with adults and work in a Neonatal Intensive Care Unit (NICU). I explored switching to dayshift when I met nurses from day shift in my cohort who wanted to work nights. However, I stopped pursuing dayshift with my manager when 1) the dayshift nurses changed their minds about working nights, and 2) I realized working the night shift was more aligned with my long-term goal to work in a NICU.
Because NICU is a specialty that people do not often leave, it is rare for any new NICU nurse to start work during the dayshift. One NICU nurse shared it takes ten years to switch to dayshift in her hospital because people never leave. I have no desire to work nights for ten years, but I am willing to work a couple of years on the night shift to work and gain experience in my dream unit. I know of a hospital in the area that supposedly has their NICU nurses move to the day shift in about 2-3 years, so my goal to to work there eventually. While I’m still adapting to working the night shift, I hope to adjust and thrive in a NICU. I’m using the time in my new grad program to adjust to the night shift, so I hopefully don’t have to struggle so much by the time I land in a NICU. I am making sacrifices now in order to reach my long-term goal to become a dayshift NICU nurse. Right now, the only way I know to get to days in a NICU is to start on nights. Hence, I continue to fight and search for ways to make night shift work for me and my family.
I would love to hear about your sleep hygiene habits and any tips for sleeping. Do you have rituals for bedtime or starting your day (or night)? What are your sleep routines? How do other parents of young children manage night shifts or graveyard shifts? What do you do to ensure you have sufficient energy while you work?
Lessons Without My Preceptor
I have been working without my preceptor since the beginning of August, or for about three weeks. I’m lucky to work in a place that values teamwork and helping one another because other nurses have helped or guided me on almost every shift since I’ve been off preceptorship. One of the biggest things I’ve learned and the best advice I’ve received as a new grad is to ASK FOR HELP.

I have no problem asking for help or clarification when I am unsure how to do something. However, I get flustered when asking someone to do things for me when I think I can or should do such things for myself or my patient. At some point in my shifts, I may start falling behind, or the unexpected happens; if I want to stay on track or not be completely off-schedule, I must ask for and accept help and support. Other nurses have started IVs or completed bladder scans at the end of my shift for me, so I can finish passing meds or complete tasks for my other patients. While uncomfortable for me, I’ve learned to ask for help and accept the support and generosity of others. (Note to self: Never mess with a funky IV contraption that ED set up – it’s probably the only way they got it to work. Trying to “fix” it just before shift change can mess it up and cause you to lose IV access, requiring a new IV start as you scramble to do morning meds).
I’m on an exponential learning curve and make mistakes. Each week, I discover new ways of doing things inefficiently, incorrectly, or in ways that doctors, patients, or my manager do not prefer. [Un]fortunately, I am learning through experience and by doing. I make mistakes or feel so uncomfortable or irritated with my performance that I must consider various ways to improve or avoid making mistakes in the future to feel competent and more confident about my work.
Communication

I’m still learning how various doctors want to communicate with nurses during the night shift. Some doctors prefer secure chat, while others only want phone calls. I’ve learned preference, of course, because I’ve utilized the opposite method of communication to what some doctors wish to use. Meanwhile, my manager advised only calling doctors in an email that I didn’t read until days after sending numerous notifications to doctors via secure chat. (I now try to be more diligent about checking my work email). Ultimately, if I need to urgently communicate with a doctor about a patient condition or issue, I will use whatever method allows me to get a hold of them. I’ve also learned that it’s better for a doctor to be upset because I communicated something they thought unimportant instead of not sharing a potential issue with a doctor. Also, I need to document every attempt at trying to reach a doctor. I had a doctor upset with me for contacting him so late in the evening, even though I called his answering service multiple times, hours earlier.
Compare and Despair
To be clear, my leadership or staff have not shamed me for my shortcomings. My leaders have been genuinely supportive and offer non-discriminatory methods of correction. I don’t feel singled out by my mistakes, and I know I’m not alone when I speak to others in my cohort. However, I measure my success by using others’ progress as my ruler. For example, one of my cohort-mates calmly activated and engaged in rapid response for one of his patients on only his fourth day without a preceptor. He received accolades from the leadership team, and our manager shared his praise with the rest of our cohort. I was so impressed and in awe by what my colleague faced and how he acted in crisis.
In comparison, during my second week, one of my patients fell. I was getting the patient’s medication in the med room when the fall occurred. Falls require an incident report and are a pretty big deal for hospitals. Thankfully, my patient did not get injured and was apologetic for the fall. I felt embarrassed and ashamed for having an incident and kept replaying the scenario and trying to understand what I could have done differently or how much worse it could have been. I have been vigilant with my patients’ bed alarms and documenting their fall education since that event.
Discovering What I Don’t Know
I have done things in less than ideal ways and made mistakes and will likely make more mistakes. However, instead of dwelling on my mistakes, I can focus on continual improvement. Am I learning from my past actions or others’ mistakes? Can I figure out how to minimize the chances for errors or prevent making the same mistakes again? Can I improve on my processes or methods? As a new nurse, I have so much room for improvement and growth. I don’t even know what I don’t know, and I keep discovering this each week.
I recently learned that I needed to administer or waste narcotics within a specific time from retrieving the medication(s) from our Omnicell. For the past three months, I dispensed and gave narcotic drugs while likely exceeding this time limit because I hadn’t known this guideline existed. I had no idea until a nurse on the floor mentioned it to me this month, and my manager emailed the team after his periodic department audit. Now that I know about this limit, I try to avoid other tasks after pulling a narcotic that may prevent me from immediately administering the medication to the patient.

Moving Forward
As I’ve shared in previous posts, I’m still adjusting to working nights and have had difficulty sleeping. I think it’s also because I’ve developed stress-induced insomnia: I replay how my shifts went and how I could have done better. I can beat myself up about things I didn’t know or events I wished I had handled differently, or I can use these experiences as lessons and move forward.

I write this blog to help others and because it allows me to process my experiences as a new nurse. It’s a way to release the ideas in my head so they don’t ruminate in my mind. My blog is also a reminder to focus on neutral or positive thoughts for self-encouragement and coaching. I consider how I would talk to a friend if they were experiencing what I was experiencing.
If you are a new nurse with anxiety before/during/after your shifts or beat yourself up over your mistakes, I am with you. Without realizing it, I survived the last night shift I had without caffeine; I think my stress response kicked in, and I was running on adrenaline. (Also, a unit secretary pointed out I was having hand tremors with the amount of caffeine I was consuming, so I’ve been trying to reduce my caffeine intake). I’m still figuring out the best ways to relieve my stress and practice self-care, just as I’m learning how to be the best nurse I can be. Besides lowering my caffeine intake, I try movement (yoga or hiking), meditating, blogging/journaling, or confiding in other nurses. It doesn’t matter how old, young, experienced, or inexperienced you are – there’s always room for growth and self-discovery.
This blog chronicles my nursing journey and serves as a journal of sorts, but I share my life to support and encourage others’ success and progress, too! I would love to hear from you: How do you give yourself grace while developing and growing? How do you move forward from mistakes? How do you practice self-care? For ideas, check out the past IG post I had about the Alphabet of Coping Mechanisms: https://www.instagram.com/p/B3uuR4ynB_9/
Staying Organized: Brains and Checklists
On my first day in Nursing Fundamentals Clinical, my instructor shared a typical schedule to follow when we’re on the floor and the expected flow of the day. My instructor explained how the nurse has to keep organized to ensure the nurse properly assesses each patient, gives medications on time, takes vital signs as needed, provides education, addresses orders, and documents care. One of my classmates asked how a nurse keeps track of everything, and my instructor responded, “Oh, I use my brain.”
My classmates looked at one another, perplexed. I wondered, “How will I hold all that information and remember everything I have to do in my brain?!?” Only later, with some further explanation from my instructor, did we realize the “brain” on which she was relying to stay organized is a document and not an organ in her body.
A nurse’s “brain” is a document that helps a nurse stay organized and allows the nurse to take notes for shift handoffs, doctor’s reports, or assessments. A nurse can also use a brain to track: treatment or surgery, when to give medications or perform additional tasks, inputs, and outputs, progression of care, or the completion of orders. Of course, the nurse documents care within a patient’s chart. However, a nurse’s “brain” serves as a mini notepad or planner for the nurse between charting.
In nursing school, I was exposed to and used various types of brains. There are numerous templates for brains available, and some are even free. During nursing school, I liked trying the brains offered by nursing.com. (With a subscription, the website provides a brainsheet database of 33 different brains, some focused on specialties like ICU, Peds, or L&D). Often, units in hospitals print specific brains for staff to use. However, it is the nurse’s preference that determines the brain a nurse uses. For instance, my preceptor never uses the unit’s pre-printed brains and writes out her brain every time she shifts. While nurses are not required to use a brain, I don’t believe I’ve ever met a nurse who doesn’t use one.
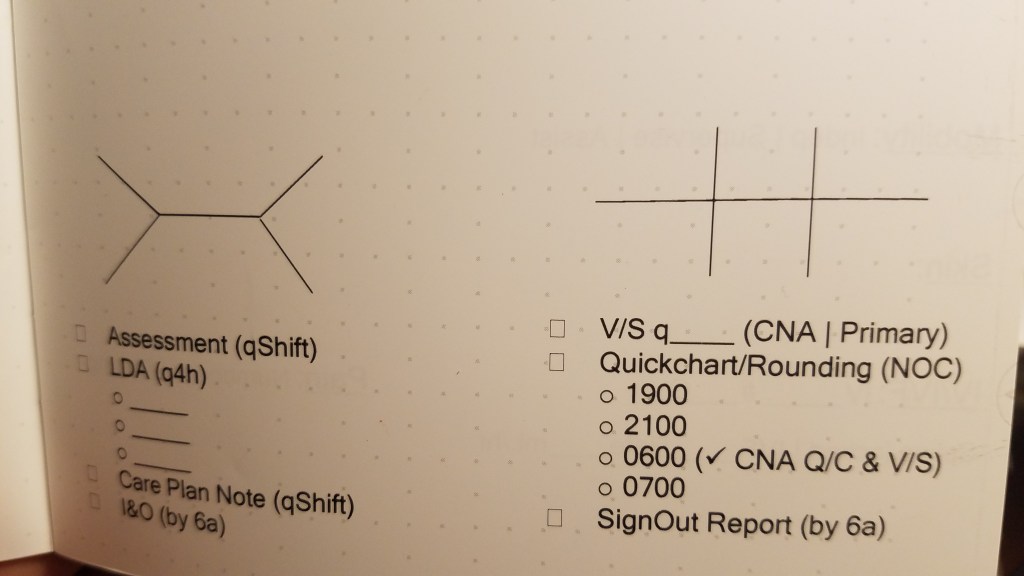
After attempting to use multiple brains, I decided to design my own. Some brains don’t have enough space, are not organized the way I want, or do not capture the information I need. As a new grad nurse, I find it difficult to track the completion of required charting or documentation unless I note it in my brain. No generic brain template is going to capture the documentation unique to my unit.
As I imagined what I wanted to include in the brain I was designing for myself, I read the book “The Checklist Manifesto: How to Get Things Right” by Atul Gawande. My husband received it as a gift, and he recommended the book to me. He thought it would interest me since the author was a surgeon exploring ways to make surgeries safer. The author worked with the World Health Organization (WHO) to develop a checklist to use for surgeries, to prevent errors (and ultimately, injuries or deaths due to preventable mistakes). It was a quick and fascinating read. He explored how other industries such as construction or airlines use checklists. As in surgery, errors in those industries can be fatal. At its worst, errors in construction or flying planes can be catastrophic and result in mass casualties. Yet, such errors are rare compared to mistakes in surgery. The book discusses how he and others developed a worldwide surgical checklist for WHO and what resulted. The author also shares when checklists are inappropriate and offers tips on developing them, even down to what font one should use. I enjoyed reading the book – it was a nice break from studying or reviewing nursing-related topics, yet I felt it was helpful to me as a nurse.
Considering what I learned from Atul Gawande, I placed a documentation checklist onto my brain template. Since I’ve set the documentation checklist in my brain, I’ve been more efficient in my charting. I can ensure I’ve completed the charting documentation for each patient without spending extra time combing through various sections of a patient’s chart to verify completion multiple times. My preceptor does not have to stay over later to complete missing documentation for our patients as she did earlier during my orientation and training. My checklist lets me know what I’ve done and what’s still missing during my shift. I know I’ve become more proficient at time management since starting orientation, but having the checklist helps me keep organized and manage my time. Plus, as a checklist gal, it feels satisfying when I cross off all the boxes in my checklist by the end of the shift.
Are there checklists you use day to day that help you in your personal life or your work? Or, are there brains you’ve used that you like? I’d love to hear and learn what works for others!
