As a bedside nurse, part of my job is to perform patient/family education. It is honestly one of the things I love to do. Since I’m in the NICU, I do most of my teaching to parents and families instead of to my neonatal patients. I can teach parents about how to care for their baby with lessons on feeding, diapering, or bathing, but I can also reinforce their understanding of their child’s diagnosis or medical condition.
At my Level IV NICU, we tend to see a lot of cardiac patients and babies born with congenital heart defects (CHD). Some of these conditions are rare and not easy to understand; even more difficult to understand without knowledge of how a normal heart works. Personally, I never knew or understood blood flow through the heart until I took anatomy and physiology. Not all our parents or caregivers have had anatomy and physiology. So how do I explain what’s going on with their baby?
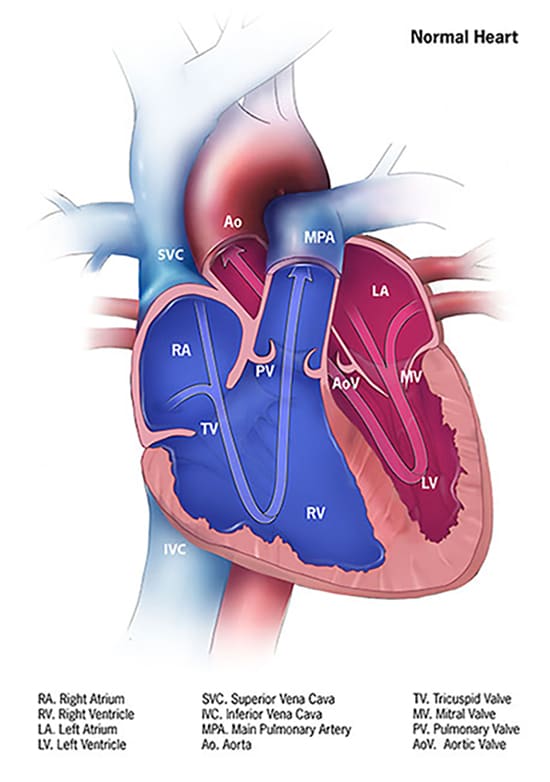
There are reputable websites I can refer to that have pictures to better understand CHD – I think they’re great for healthcare professionals and nursing students as well. One of them is the Centers for Disease Control and Prevention https://www.cdc.gov/ncbddd/heartdefects/index.html.
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
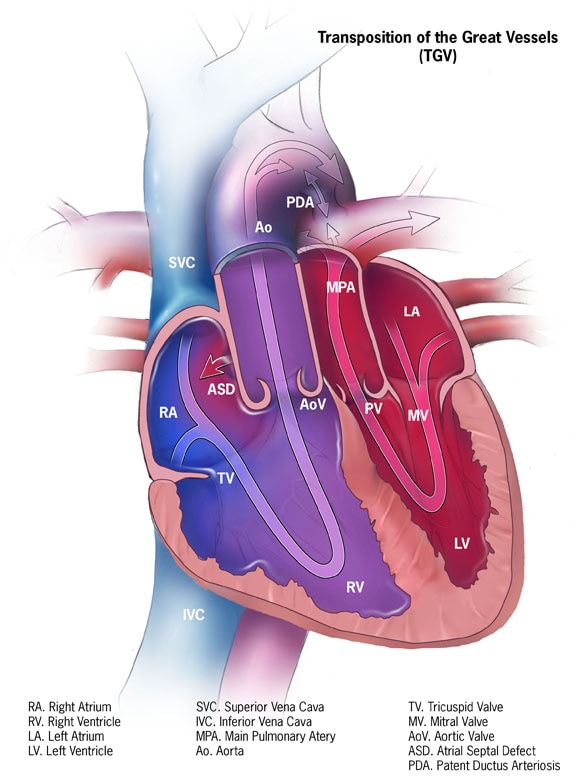
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
Another website that’s a great resource for CHDs is Cincinnati Children’s https://www.cincinnatichildrens.org/service/c/cardiothoracic-surgery. Cincinnati Children’s even offers animated heart videos to illustrate various heart conditions. While I love and recommend these resources, I’ve been wondering how I could further simplify patient teaching. In nursing school, I was taught to conduct patient teachings at the 5th grade level. Healthcare professionals should simplify teaching to their patients and patients’ families and use words such that a 5th grader could understand.
Recently, I’ve been thinking about teaching for a family who had a baby come to our hospital with a rare congenital heart defect, Transposition of the Great Arteries (TGA, or d-TGA). They seemed hesitant in explaining their child’s condition. They held up their hands and shared their baby’s arteries need to be like this (as they held their hands up, crossed like an ‘X’) but that their baby’s arteries are like this (as they held their hands parallel) to each other. They were not wrong in their explanation, but I wondered if they understood why it needed to be “crossed”. I felt like a process diagram could have been helpful.
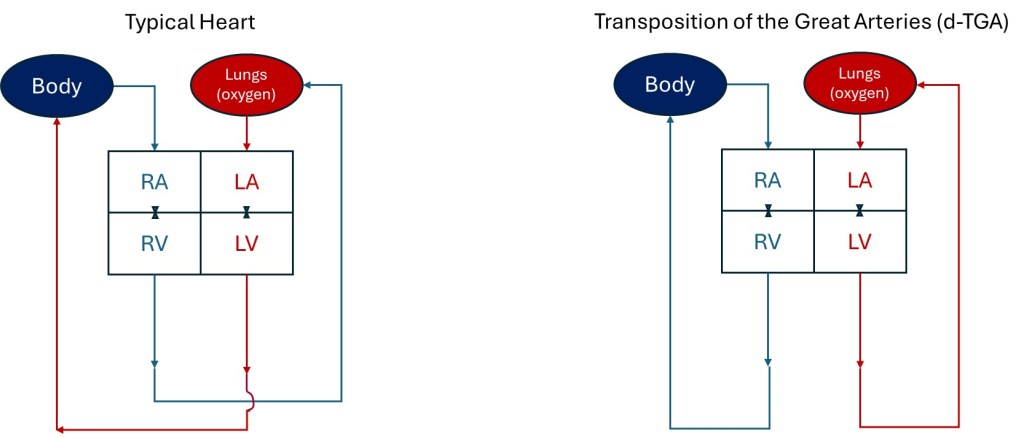
As a former engineer, I used to make flow charts in either designing or explaining existing manufacturing processes. I really wanted to simplify the explanation of blood flow to /from the heart with a process diagram. I drew it out when I got home and then tried to replicate what I drew on the computer. Below are the process flow diagrams I designed, using the same abbreviations as the CDC used to describe parts of the heart in their diagrams: RA = right atrium, LA = left atrium, LV = left ventricle, RV = right ventricle. I also used red to represent oxygenated blood and blue to represent oxygen depleted blood. I represent the tricuspid and mitral valves with the valve graphics used in engineering diagrams. I drew the little curve on the Typical Heart drawing to show the vessels leaving the heart don’t intersect/mix as they cross one another.
Process Flow Diagram representations of the typical heart flow compared to a heart with d-TGA
It’s not an accurate anatomic representation with size and doesn’t depict all the ways the blood enters the heart or how the arteries go up and out of the heart. The vessels and all the valves aren’t even labeled, but I think it easily shows why TGA is such a critical heart defect. From my flow diagram, I think it’s clear the rest of the body can’t receive oxygen with d-TGA because blood from the lungs can’t be delivered to the rest of the body. As a healthcare professional or nursing student, I love the CDC and Cincinnati Children’s images to explain the heart and defects. However, as an engineer, I love the simplicity of my flow diagrams.
If you were a 5th grader, what graphics are easier to understand? What do you think about my depictions? For my next blog post, I’ll share the diagrams I made that show how a baby survives d-TGA until they receive surgery to switch the arteries and correct the flow to the lungs and body. Hint: Look at the ASD and PDA in the CDC graphic for the TGV heart.
To my dear nurses & nurses-to-be: Happy Nurses Week, and thank you for all that you do! It’s nice to get gifts and swag during Nurse’s Week, but I hope you’re appreciated every day!
Update on me: I’m still on orientation at my new hospital. I worked Sunday through Wednesday this week as well as celebrated my daughter’s birthday, so I’ve been busy. For Nurse’s Week, I got to enjoy a goody bag, free breakfast, free drinks & snacks, and I got to experience a mini massage, reiki, and sound bath session at work. At my hospital, they have a nurse’s MONTH! I’m hoping to take advantage of the fun or relaxing activities they have to offer beyond this week…not sure what that is yet.
Throughout social media, I’ve seen some funny or questionable gifts for nurses in celebration of nurses week…Even if you don’t get the best gifts or activities for Nurse’s Week, I hope you are happy in what you do and feel properly compensated for your nursing role. I myself have high and low days, but am overall happy with my decision to be a second-career nurse! Good luck on your journey!
Part of my attraction to becoming a nurse was being able to spend more time with my family. Most nurses I knew worked only three days a week, allowing them four free days to do what they wanted each week. I also appreciated that bedside nurses do not take their work home. Most bedside nurses are not on-call or still working when they come home. In my previous engineering career, I worked five days a week and was at work much longer than just eight hours a day. I would sometimes work night shifts and weekends. I was on call frequently or still worked even while home or on vacation. The thought of being free of the tether of work appealed to me as I pursued my career change to become a nurse. Now that I’ve been a bedside nurse for a few years, do I still feel nursing is as family-friendly as I initially thought?
12 hour Shifts
Like most bedside nurses, I am at work 12.5 hours every shift. (Most nurses who work 12-hour shifts are at their place of employment for 12.5 hours due to an unpaid 30-minute meal break). After adding commuting, showering, eating, and sleeping to that schedule, I can do little else on the days (or nights) I work. When I work, I see my daughter for only about an hour each day, regardless if it’s the day or night shift.
When I work days, I must leave the house before my daughter wakes to be at my hospital for a 7a shift. Dayshift ends at 7:30p, and if my commute is nice and short, I get home around 8p. I shower and eat as soon as I come home, but I don’t get to eat dinner with my daughter because it’s too late for her. I have about an hour at home before my daughter’s targeted bedtime at 9p.
When I work nights, I leave the house around 6:15p (since my commute for my new job is shorter now) to start my shift at 7p. My night shift ends at 7:30a, and I get home around 8a. I don’t usually see my daughter when I come home from nightshift because she gets to school before 8a. I shower, eat, and sleep. I target sleeping until 5p. If I get up earlier and my daughter comes home from aftercare before our usual pick-up time, I can spend about an hour with her before I get ready and leave for work.
If I break it down, there isn’t an ideal [12-hour] shift schedule to spend more time with my family on the days/nights I work. Dayshift may be slightly better because I don’t need a sleep/recovery day on my day off as I do after working a night shift. The real advantage of my 12-hour shiftwork is that I don’t have to work as many days each week as in traditional jobs.
Three Shifts Per Week
I can work three 12-hour shifts per week at my current hospital and be considered a full-time employee with benefits. (My prior hospital required a fourth shift one week per month to be considered full-time). Working only three days (or nights) per week means I can have more family time on my four days or nights off that week. The three-shifts-a-week schedule was beneficial for an unplanned trip at the end of March.
Unexpectedly, my husband’s last living grandparent died last month. The funeral service was in Hawaii on a Saturday morning. I hoped to go and support my husband and his family, but I needed to figure out if I could join him since I had just started my new job and had no vacation. My daughter could join him since the trip was during her Spring Break.
Due to my night shift nursing schedule, I joined the family in Hawaii without asking for time off of work. I worked a Thursday night shift – my third shift in a row – and packed as soon as I got home Friday morning. We left that same Friday afternoon and returned home on an overnight flight Wednesday night / Thursday morning. When we returned from Hawaii Thursday morning, I slept and went to work that evening – my first of three in a row. It was a grueling schedule, but I would not have been able to travel with my family for six days without needing time off if I had still worked as an engineer. What other jobs would allow for a personal 6-day trip within 1.5 months of starting?
I was (and still am) on orientation. I did not select my schedule to plan my trip. My supervisors set my schedule to match my preceptor’s. Fortunately, it worked out for me to travel to Hawaii without missing or rescheduling my orientation.
Though it was unplanned and under sad circumstances, my spouse, daughter, and I enjoyed spending time with extended family on our recent trip to Hawaii. I appreciate that my schedule allowed me to travel without taking time off. This pic was taken during on a coastal hike to Makauwahi cave. The hike to Makauwahi cave splits off to a secluded beach. Though my husband and his family had been to the Kauai many times, they had never been to the cave. It was nice to join them in discovering new sites on the island. More importantly, I appreciated being able to celebrate the life of my husband’s maternal grandmother and support him, and be there for family.
I know many other nurses who plan extensive trips on their days between work or by taking only a handful of vacation days. A nurse working three shifts a week could schedule themselves such that they have eight days off between work shifts with no personal time off used. In my previous career as an engineer, I would only have been able to miss work for eight days in a row if I had used vacation days or other forms of leave. The one major caveat to getting desired days off without using vacation or personal time off is nurses still need to get their schedule requests approved or be able to self-schedule. Every nursing job I’ve had allowed me to self-schedule, but I know other nurses who don’t get to select their schedules. My supervisors granted my schedule requests about 98% of the time in my past jobs, so I mostly worked the days/nights I chose (once I was off orientation).
Heavy Workload
When determining if a nurse’s schedule is family-friendly, something else to consider is how much downtime one needs between shifts to recover from work. To schedule a block of days off, as I described above, one usually needs to work a block of days before and after, which can be exhausting. As a night-shifter, I need the day off after work to sleep or nap. My first day off after a block of night shifts is not a day I expect to spend much (awake and alert) time with my family. However, I’ve also had days after working some day shifts where I’ve felt like a zombie. I’ve never felt as drained (emotionally, mentally, and physically) after working as I do as a nurse. I’ve discussed this before in past posts and how sometimes I need a day or two to recover from shift work. Being an engineer could sometimes feel draining, but it was not consistently exhausting compared to being a nurse.
Weekdays Off
Despite needing recovery days, I like having weekdays off as a bedside nurse because it allows me to participate easily in some of my daughter’s school activities. My schedule has allowed me to attend 20-minute in-person parent-teacher conferences in the middle of a weekday afternoon without taking time off from work. I attended my daughter’s award ceremony on a random weekday morning I wasn’t scheduled to work. If my time off coincides with my daughter’s breaks or early dismissals from school, I get to spend time with her exploring our city and going to parks or museums instead of placing her in hard-to-find, expensive camps. I can attend weekday medical or dental appointments for myself or my daughter without taking any time off when I schedule them on days/nights I’m not working.
Weekends & Holidays
While it’s nice to have some weekdays off each week, my schedule requires me to work weekends and a handful of major holidays. I miss spending about half the weekends with my family every month due to work. I have to celebrate Thanksgiving or Christmas early or late if I want to celebrate with family. Some senior nurses at my last job managed to get out of working significant holidays, but no one got out of having work weekends. My current preceptor has worked for over 20 years, but like me, she must work four weekend-shifts each month. Even though I gained some flexibility for weekday activities, I lost spending half my weekends and holidays with family when I switched careers.
Working from Home
Another thing I lost when I became a bedside nurse is the ability to work from home or remotely. I must take time off work if I’m sick, in quarantine, or my daughter is ill (and I stay home with her instead of my husband). I cannot do my job and care for my patients remotely. Remote nursing jobs exist, but not for bedside nurses. On the other hand, being unable to work remotely can be a positive thing for work-life balance because it allows me to separate from work compared to when I was an engineer.
Wait – Let me rethink that. One day in Hawaii, I attended paid mandatory training for my orientation. And if I’m being candid, I spend hours of unpaid time reviewing topics or concepts to prepare for work when I’m not at work. Education and review is my coping mechanism for the stress I face as a novice nurse. Educating myself or doing unpaid training outside of work may persist even as I become more experienced. Nursing requires continuing education. However, I’m genuinely interested in learning about my patient population and ways to provide the best care or be a better nurse. There are always new techniques, equipment, or updated evidence-based practices to learn. I can only sometimes research or learn about new nursing practices during work hours. So there may not be a complete separation from work when I leave the hospital, but it’s an improvement compared to my life as an engineer.
Job & Schedule Variety
I wanted to accurately portray what it’s like to work as a bedside nurse while having a family with this post. However, if a bedside nurse chooses, they do not have to work the traditional three 12-hour shifts per week that I do. Bedside nurses can have one or multiple per diem (one day a week) jobs or work 8 hours a day, five days a week (my last hospital offered 8-hour shifts on the Post-Partum unit). Or, bedside nurses can become travel nurses and work 13-week contracts or whatever they choose to negotiate. There are so many scheduling options out there for nurses. A nurse doesn’t even have to work bedside! A nurse can select a job or schedule that works best for their family and personal life.
The Reality
While nursing can be appealing due to the work schedule, I wanted to review the reality of balancing family and work as a bedside nurse. Despite some drawbacks, my nursing schedule can be family-friendly overall. Is my bedside nursing schedule MORE family-friendly than when I was an engineer? Nope. But I love being a nurse. I love working with my patients and their families and learning, teaching, and helping others. If you are considering nursing as a profession, I hope this blog post gives you a better idea of what a nursing schedule is like and if this profession will allow you to balance work with your family or personal life. Good luck on your journey!
How do you manage stress? Attending school as an older student or pursuing a second career can be stressful. Being a caregiver for aging parents or other family members while working and taking classes can be stressful. Trying to balance parenting and being a nursing or pre-nursing student can be stressful. Do you have a strategy for handling such stress?
My work enrolled me in training last year, where this stress buster wheel was presented and discussed. The stress buster wheel captures evidence-based strategies for toxic stress intervention. The training was for caregivers and healthcare workers to screen and treat patients for Adverse Childhood Experiences (ACEs). However, the stress-buster strategies are an excellent reference for anyone experiencing stress. Do you employ any of these strategies for yourself? Are there ones you’d like to try or implement more?
I like combining several stress busters by going on garden walks or hikes through nature with friends. I connected with a friend (outside of school or class) at least weekly during nursing school to maintain supportive relationships. This helped bring balance into my life, especially when I sometimes felt consumed by my intense 15-month accelerated BSN program. Now that I’ve graduated, I continue this practice to connect with friends regularly.
I viewed this coaching/motivational video (https://www.youtube.com/watch?v=oDzfZOfNki4) by Duke Women’s Basketball’s Kara Lawson about how we need to “Handle Hard Better.” I share this post and video to motivate you as we reflect and head toward the weekend. Things get more challenging as we grow, develop, and learn. We become more skilled and adept at facing what’s in front of us. Again, things didn’t get easier – we just got better! We learned to handle hard better.
Another way to look at it: Walking was once difficult, but once I mastered that, I learned to use the stairs, jump, and eventually run. Once we become comfortable handling what we once thought was a challenge, it’s time to take on a new challenge to continue our growth and development. I didn’t even get “comfortable” with my old job or feel like I “mastered” it, yet I left and started a new one! I left my previous NICU (Level 2) to move to a higher acuity NICU (Level 4) because I knew I wanted to be able to handle more seriously ill patients.
I completed my first week with my preceptors at my new job, and it was a little overwhelming. Moving from a Level 2 NICU to a Level 4 NICU feels like a big jump. There’s so much to learn! In some ways, I feel like a new grad nurse all over again and have to familiarize myself with new equipment, processes, and diseases for my higher acuity patients. The video is a reminder to “handle hard better.” The way I handle hard better is to practice and expand my skills and to be willing to learn and open to coaching. I reflect on my performance and search for ways to improve. The way I handle hard is to do what I can to make myself better.
What does that look like for me? I am making report sheets or brains that work for me on my new unit and make me more efficient. I am learning about different disease processes by reading about them and watching YouTube videos. I am giving shift report even though I don’t feel like I’m ready because “doing” is better practice for me than “watching”. I’m learning the new charting system and what my new hospital requires for each shift. I’m learning about the workflow and general day-to-day schedule and expectations. I’m reflecting on my week by writing this post…and I’m giving myself grace that I’m still learning and will improve with more practice and time.
You may be hesitant to pursue a new job or career. You may be reluctant to go back to school. I am here to encourage you. I have met many second-career nurses, older students, and moms returning to college or joining nursing school since I became a nurse. My story is not unique. I share my life as a second-career nurse hoping to inspire others to pursue their dreams even when circumstances may seem hard. You can do it – you can “handle hard better”! Good luck on your journey!
NICU nurses in my hospital are responsible for putting IVs in our neonatal patients. We don’t have an IV team to do it for us, and often, our nurses are called to other units when other units have difficulty putting IVs in babies. Regardless, IV placement is an essential nursing skill, and putting IVs in infants is different than putting IVs in adults. For adults, I can usually see or palpate (feel) veins. For babies, it can be difficult to see veins, and I’ve never been able to palpate them. It had been a while since I placed an IV in a baby, so I asked and volunteered to do it for a colleague needing to replace an IV in her patient on my last shift.
I placed the IV in the patient, but not without almost giving myself a needle stick (I dropped the needle, and it rolled away from me before I could retract it) and having some blood splash from quickly releasing a used hub on a bedside table. I’ve never come close to giving myself a needle stick, nor have I created such a mess from attempting to place an IV. Senior nurses were present to help me hold down the baby and hold up a vein finder. I felt like I was fumbling through the process with an audience. I hadn’t worked with these nurses before to place an IV because I was still new to the night shift. And while I eventually got the IV in, I felt foolish with how long it took and how I splashed blood on the table. I’m embarrassed that this is the first impression I’ve given these nurses on my IV skills. In a way, however, it was confirmation that I needed the practice.
While I was placing the IV on my colleague’s patient, the IV on my patient stopped working and needed replacement. As soon as I placed the IV on my colleague’s patient, I hurried to my patient’s isolette. I attempted to put a new IV on my patient, got it during my second attempt (the vein blew during the first attempt), but then accidentally pulled out the catheter as I tried to remove the tape and Tegaderm to retape the IV. It had stopped flushing smoothly, and the other nurse and I thought we could retape it to prevent it from getting kinked or occluded. As a guideline, a different nurse should take over the IV placement after two unsuccessful attempts. I stopped with further IV attempts on my patient beyond my two tries but got the lesson to remove tape individually so as not to pull out an entire catheter when retaping. (I had initially tried pulling off the tape before the Tegaderm, but it was hard to separate it from the Tegaderm). My colleagues eventually got a new IV in my patient. I appreciate the teamwork, but I still feel embarrassed by how I kept “messing up.”
I wanted IV practice on my last shift, and the universe gave me multiple chances! As humbling as my previous shift was, I realize the only way to improve my nursing skills is with experience and practicing essential skills: I will be more consistent and successful at putting in IVs only by putting in more IVs. Luckily, NICU nurses support each other and help and assist one another during IV placements. However, there are times when the unit is busy, and nurses may not always be available to help each other. I want to feel more confident with doing IV placement alone. I will have to request to do IVs whenever there is a chance.
Sometimes, it feels weird to be older and yet so new in work experience. I must remind myself and give myself the grace that I am still relatively new to my profession. There’s a lot I’m still learning to do that senior nurses do effortlessly and automatically. And even the most experienced nurses make mistakes or are sometimes unable to get an IV placed on the first try. I can’t expect perfection, but I can at least aim for improvement.
Across the country, the school year has started for many college students. Students might wonder how to stay organized or manage their time. When I began the journey to become a second-career nurse, I was balancing school, work, parenting, and my personal life. Having a planner was critical for me to manage my time. Below is a list of seven things I included in my planner and recommend students to include in theirs – the last one may surprise you!
Class times. Put in all your scheduled lectures, discussion sections, clinicals, & labs.
Class dates of quizzes, exams, and project due dates. Take the syllabus at the beginning of the semester or quarter and jot down when all the quizzes, exams, practicums, & project deadlines are taking place. Use a different color or shape to identify these in your calendar quickly. I would use blue for quizzes and red for exams or significant projects. The color coding allowed me to easily see when something was coming up and when I needed to study or prepare for something that would impact my grade.
Commute time. I live in Los Angeles, and sometimes commutes can take an hour or more to/from school or work. It’s important to factor this in if commutes can be lengthy in your area, especially if you are responsible for daycare or preschool drop-offs & pickups. Remember to factor in parking as well since that may add to the time it takes to get to a destination. Some people have to park in a garage or lot far from the building where they work, have classes, or have clinical. One of my clinicals took place in a hospital that was a 15-20 minute walk through a tunnel and stairways from the parking lot where we were assigned. If you forget to factor in the extra time it takes to park and walk to your destination, you can end up being late.
Other family members’ schedules. Your family’s schedule is essential. I put in when my parents need me to give them rides to doctor’s appointments or dental procedures. I also add my husband’s business trips (meaning I’m single-parenting my daughter while he travels) or when my daughter has dance, sports, religious education, classmate birthday parties, or school events.
Meals, sleep, & shower/hygiene schedule. If you need 6-8 hours of sleep to function, make sure you schedule it in your calendar. I say this because my targeted bedtimes would sometimes surprise me based on how early I’d need to get up for my commute, etc. Sleep schedules are also important to note if you have children or other family members who require your help to get ready for bed or to get ready for their day.
Study time. The other mom in my nursing program and I found it challenging to study at home once our kids were out of school. I sometimes booked a private room in a library or computer lab to study. Mostly, I would use my spare time to read or do homework between classes or before class if I arrived at school early. I recommend scheduling studying time to realistically determine how much time you have to study, especially if you have other competing obligations such as family or work.
Events or activities that nourish me or bring me joy. I also color-coded these events or activities to quickly glance at my calendar and see that I planned something fun each week. This one activity was not an obligation or part of a busy to-do checklist of duties. It was something I looked forward to doing and had nothing to do with school. I recommend including at least one weekly activity that replenishes you and brings you joy or comfort. Make it happen. The activity could be family game night, happy hour, facetime with a long-distance friend, attending a party, reading a book, yoga, hiking, painting, baking, massage, seeing a musical, or going on a mini-retreat. Each person has different interests and things that bring them joy. Make sure you know what that is for yourself. Ensure you are doing something for yourself at least once a week that helps you reset. You may be a student balancing many things in life, but you’re not a robot. You are a human and have other interests and desires outside of school. Make sure you regularly do things that light you up!
When I had my baby, my husband and I struggled to feed our newborn. I wanted to breastfeed my baby exclusively, but she would not breastfeed well. Influenced by various sources and committed to breastfeeding, I refused to pump or bottle-feed my baby while in the hospital. My baby and I roomed in together while I tried to breastfeed. My husband recalls having to travel with my baby somewhere for light therapy. I vaguely remember this too, but I was tired, delirious from lack of sleep, and recovering from a C-section. I only remember sleeping while my husband and baby were out of the room. In retrospect, my baby most likely went to the NICU because she was jaundiced. She may have been there for only a few hours because I remember waking when my baby and husband returned from wherever they went. Thankfully, the hospital did not admit my baby to the NICU, and we could leave the hospital together. However, our struggles to feed our newborn continued when we got home. Looking back at our experience as new parents, I wish I had known some things about feeding our baby that I know now as an experienced mom and NICU nurse.
Photo by Helena Jankoviu010dovu00e1 Kovu00e1u010dovu00e1 on Pexels.com
Fed is Best
As a NICU nurse, I see term or late pre-term infants (born at 34-37 weeks gestation) who come to our NICU for hypoglycemia (low blood sugar) or hyperbilirubinemia (seen as jaundice/yellowish skin). Often, these term babies come to our unit because they are not eating well. For some babies, parents refuse to feed baby formula while postpartum, and the mom may not have established her breastmilk supply yet. This description reflected us as newborn parents and a likely reason why my baby needed phototherapy.
A build-up of bilirubin in a baby’s body can cause jaundice. Bilirubin is usually processed by the liver and leaves the body as waste. A newborn’s liver may not yet efficiently function, but the baby should be eating/drinking something to produce waste and encourage processing out bilirubin. A newborn baby drinking breastmilk or formula helps curtail jaundice. If a baby is not feeding well or is still jaundiced despite attempted feedings, however, hospitals can treat elevated bilirubin levels (hyperbilirubinemia) through light phototherapy.
Jaundice is normal in newborns, but the hospital monitors bilirubin levels and treats when levels rise above certain thresholds. If the baby’s bilirubin is too high, brain damage can occur. In our hospital, if a postpartum baby needs phototherapy, the baby is admitted to the NICU. Phototherapy in the NICU only happens after multiple attempted feedings and when bilirubin levels exceed treatment thresholds.
Frequent feedings are how parents can reduce bilirubin levels in otherwise healthy babies (and hopefully prevent hyperbilirubinemia that requires NICU care). However, frequent feedings can also help prevent another common condition in our NICU: hypoglycemia, or low blood sugar. If an otherwise healthy baby born to a non-diabetic mom takes enough breastmilk or formula, the baby can usually avoid hypoglycemia. However, if the baby is unable to feed adequately, the baby can develop low blood sugar.
Before a baby goes to the NICU for hypoglycemia treatment and monitoring, the mother and the postpartum staff will attempt to feed the baby. If the mother consents, the baby can be offered formula. If bottle-feeding is still insufficient, a sugar gel is given to the baby orally. The postpartum unit will attempt several feeding and sugar gel administrations before the baby goes to the NICU. If the NICU admits a baby for hypoglycemia, we will place an IV to deliver sugar to the baby as IV fluids. Once the sugar levels in the baby are sufficient, and the baby is drinking adequately, we can reduce the IV fluids and eventually remove IV fluids if the baby can orally consume the needed calories and fluids while maintaining healthy blood sugar and hydration. In the NICU, we try feeding our babies breastmilk if it’s available and not contraindicated (i.e., substance-abusing mother). If breastmilk is unavailable and we need to feed a baby orally, we will give provider-ordered formula to our babies.
For babies admitted for hyperbilirubinemia or hypoglycemia, I sometimes hear the baby barely drank anything because the baby was unable to breastfeed from a mom who wanted only to breastfeed exclusively. Before doctors send the baby to the NICU, the nurses can offer the baby formula if the mom consents or requests it. However, by this time, the baby may have worn themselves out or be too tired to drink from the bottle. It makes me and other NICU nurses wonder, “If the parent or nurses fed the baby from the bottle sooner, would the baby still need to go to the NICU? Is the mother promptly informed of her options if her milk supply hasn’t come in or the baby cannot latch or breastfeed?”
While I’m glad my husband got to go with my baby and accompany her for phototherapy, I would have preferred that my baby not leave my postpartum room at all for treatment or tests. To prevent my daughter from needing to leave our room, I would have pumped sooner to encourage my milk supply and produce milk that my husband or I could bottle-feed my baby. We did not learn until weeks later that my daughter was tongue- and lip-tied, which may have initially made it difficult for her to breastfeed. From my perspective, it’s better to feed a newborn some formula to keep the baby with mom and out of the NICU than to rely solely on breastmilk that may not be available yet or difficult for the baby to access.
Pumping is Okay
I was offered to pump in the hospital but refused, thinking I would breastfeed. My doula recommended not to pump until after the first month, so I tried holding off on pumping in an attempt to have my baby latch, help establish our breastfeeding rhythm, and set my breastmilk supply.
I didn’t want to feed her from a bottle because I didn’t want to cause nipple confusion and have my baby prefer the bottle over breastfeeding. When we got home, I thought I was doing okay breastfeeding, but when we brought our baby to her 1-week checkup, she wasn’t gaining enough weight. We brought her to her 2-week checkup, and her pediatrician still didn’t think she was gaining enough. My daughter fell in the 2nd percentile on the growth chart. (I did not discover until months later that my husband and his siblings were so small as newborns they were not even on the growth chart). We were strongly encouraged to start bottle feeding her formula.
Wrought with guilt, we decided to feed her some formula, and I began to pump. By this time, I had developed mastitis (Mastitis is a painful infection in the breast caused by bacteria introduced by breastfeeding. It also caused me to have body aches, a high fever, and chills. Imagine dealing with this while trying to care for a newborn!) My supply was woefully insufficient, and most of my daughter’s caloric intake was formula once I started to pump while battling mastitis.
Formula is Okay
It is okay to use formula if you are not producing breast milk or enough breast milk/colostrum to feed your baby. I wanted to exclusively breastfeed because I learned about the benefits of breastfeeding and how it’s the best, natural, and easiest way to feed my baby. It’s great for baby bonding and helps provide passive immunity to the baby. However, I got mastitis TWICE within the first month or so of my daughter’s life. We also learned my daughter was tongue-tied, making it difficult for my daughter to breastfeed. Not until later did I meet other mothers who breastfed AND bottle-fed their babies or moms who exclusively pumped. (Moms who exclusively pump only feed their babies breastmilk from a bottle). Had I not been so attached to exclusively breastfeeding, I could have adapted and explored these other options earlier as a new parent.
Do What’s Best for You and Your Family
Aside from taking antibiotics, the way to clear a mastitis infection from the breast is by breastfeeding or pumping. My daughter preferred the bottle by this time, so I relied on pumping to clear my infection. Pumping (and antibiotics) eventually relieved the pain and released the mastitis in my breasts, but the repeated infections impacted my supply. Encouraged by my doula, I remember three days where I spent about 9 hours pumping (diligently pumping 45 minutes every 2 hours, per her recommendation) only to produce about 1 ounce of breastmilk daily. I was so exhausted and upset by the results of my efforts. I also felt cut off from my daughter while I pumped (Because I couldn’t figure out how to safely hold her with all the pumping tubes hanging from my body, my husband or parents would take her while I pumped). After the three days dedicated to pumping round-the-clock, I decided it was not worth it to continue to pump. It was more important for me to be with my baby than to try giving her my pumped breastmilk.
I still held out hope for breastfeeding. Once my infection cleared, I tried to breastfeed my daughter using an SNS (supplemental nursing system – a tube placed on the breast but connected to a bottle to measure and ensure the baby has adequate intake). She was already used to the bottle nipple and did not take to the SNS. I attempted multiple times, but she would refuse to feed through the SNS, and I would end up with formula spilling all over my chest.
I share a bit of my breastfeeding journey to emphasize that there are many ways to feed and nourish a baby. In the end, so long as the baby is healthy and safe, parents decide what works best for them and their family. The caregivers’ mental health and well-being are as important as the baby’s. The way you choose to care for your baby may not resemble how other families do things, and that’s okay. I was ashamed for not breastfeeding my daughter for as long and in the way I hoped, but I felt my attachment to breastfeeding distanced my baby from me and caused so much anxiety and distress. Parents should not be ashamed of doing what is best for them and their families.
In the NICU, I meet moms who feel nervous they cannot directly breastfeed, yet they can pump and produce enough breastmilk to meet their baby’s needs. I meet parents who are ashamed they don’t have a separate nursery for their baby. We live in Los Angeles – not every family can afford to pay for a home with different bedrooms for each of their children! Many of our parents rely on WIC because they can’t afford to purchase formula. Getting formula from WIC is better than diluting formula or not feeding the baby enough nutritious calories. I try to assure the parents I see they can do what works for their family – it doesn’t need to match other families.
I felt defeated when I finally gave up pumping and breastfeeding. I wish I gave myself a little grace as a newborn mom and wasn’t so hard on myself. I felt so much grief over my inability to mother and feed my child as I thought I should that it made me feel inadequate as a mom. I was separated from my baby while I pumped, trying to salvage any breastmilk I had. I cried every day when I was pumping or trying to breastfeed. Ultimately, I fed my baby adequately, thanks to formula, and my child is now a healthy school-age girl. She still falls on the low end of the growth chart, but her father and I are not tall, so my daughter’s standard is the tenth percentile or less.
As I reflect on my experience as a new mom, I hope to impart grace and support to other new parents now that I’m a NICU nurse. If a caregiver is feeding their baby adequately, caring for and bonding with them, and keeping them safe, I want them to know they are doing a great job! I also want them to know it’s okay to make adjustments as needed or change their minds about how they want to do things. Parents can adapt their plans according to the family’s needs.
I originally wrote this post to give insight on how to lower the likelihood of hyperbilirubinemia or hypoglycemia (and admission to the NICU) through frequent feedings. If this information helps reduce NICU admissions and prolong in-room bonding between caregiver and baby, I would be ecstatic. Ultimately, I hope this post reassures parents (and serves as a reminder to myself) that there are many ways to care for a baby. There are no perfect parents; there are no perfect children. We’re just doing our best with the information and resources we have. Good luck to you on your journey!