As a bedside nurse, part of my job is to perform patient/family education. It is honestly one of the things I love to do. Since I’m in the NICU, I do most of my teaching to parents and families instead of to my neonatal patients. I can teach parents about how to care for their baby with lessons on feeding, diapering, or bathing, but I can also reinforce their understanding of their child’s diagnosis or medical condition.
At my Level IV NICU, we tend to see a lot of cardiac patients and babies born with congenital heart defects (CHD). Some of these conditions are rare and not easy to understand; even more difficult to understand without knowledge of how a normal heart works. Personally, I never knew or understood blood flow through the heart until I took anatomy and physiology. Not all our parents or caregivers have had anatomy and physiology. So how do I explain what’s going on with their baby?
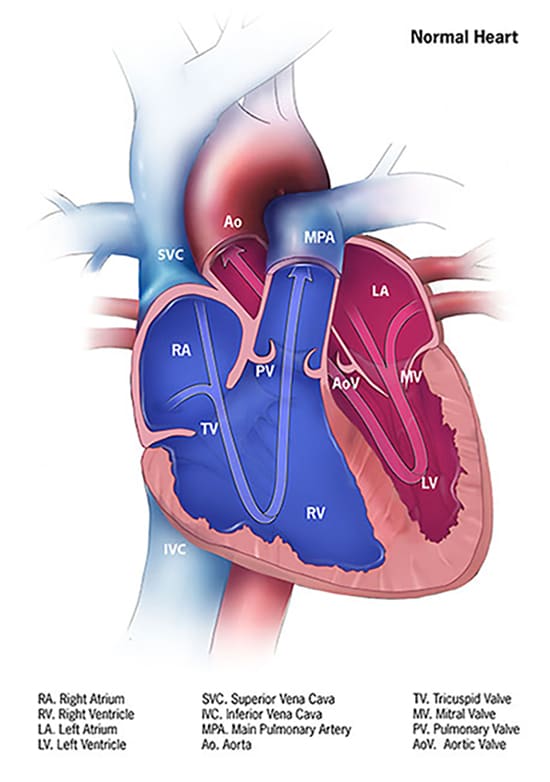
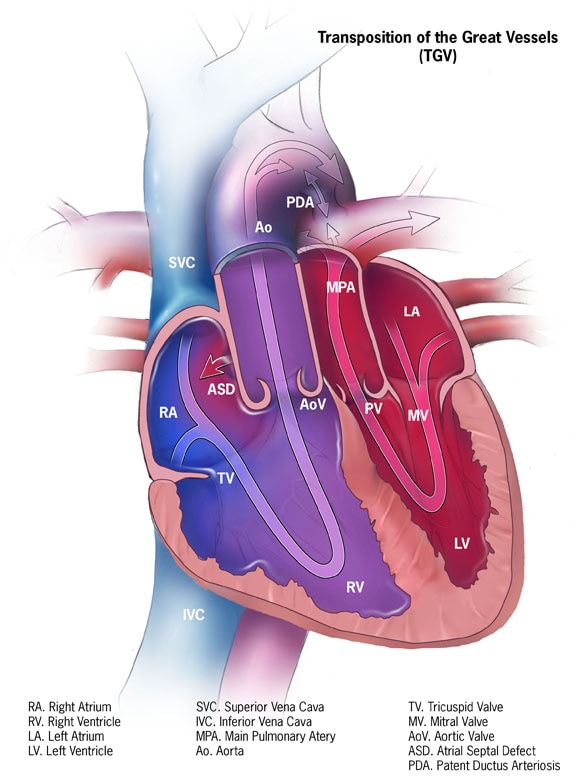
There are reputable websites I can refer to that have pictures to better understand CHD – I think they’re great for healthcare professionals and nursing students as well. One of them is the Centers for Disease Control and Prevention https://www.cdc.gov/ncbddd/heartdefects/index.html.
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
Another website that’s a great resource for CHDs is Cincinnati Children’s https://www.cincinnatichildrens.org/service/c/cardiothoracic-surgery. Cincinnati Children’s even offers animated heart videos to illustrate various heart conditions. While I love and recommend these resources, I’ve been wondering how I could further simplify patient teaching. In nursing school, I was taught to conduct patient teachings at the 5th grade level. Healthcare professionals should simplify teaching to their patients and patients’ families and use words such that a 5th grader could understand.
Recently, I’ve been thinking about teaching for a family who had a baby come to our hospital with a rare congenital heart defect, Transposition of the Great Arteries (TGA, or d-TGA). They seemed hesitant in explaining their child’s condition. They held up their hands and shared their baby’s arteries need to be like this (as they held their hands up, crossed like an ‘X’) but that their baby’s arteries are like this (as they held their hands parallel) to each other. They were not wrong in their explanation, but I wondered if they understood why it needed to be “crossed”. I felt like a process diagram could have been helpful.
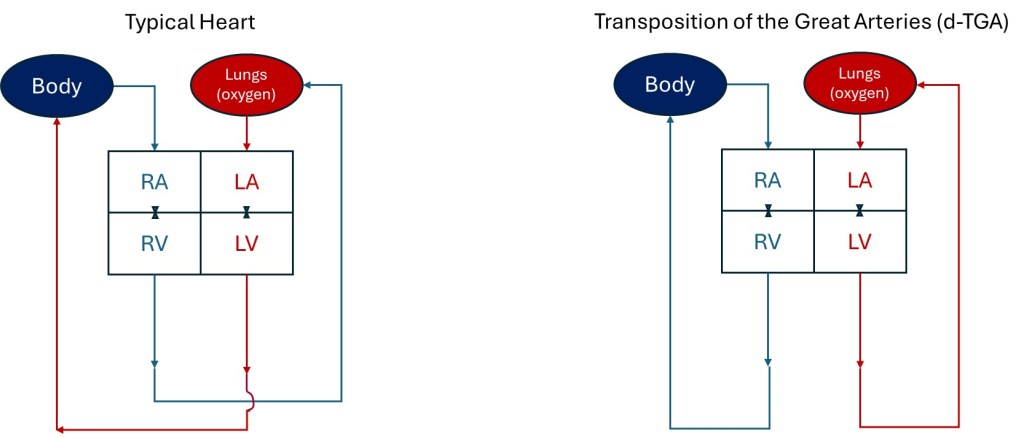
As a former engineer, I used to make flow charts in either designing or explaining existing manufacturing processes. I really wanted to simplify the explanation of blood flow to /from the heart with a process diagram. I drew it out when I got home and then tried to replicate what I drew on the computer. Below are the process flow diagrams I designed, using the same abbreviations as the CDC used to describe parts of the heart in their diagrams: RA = right atrium, LA = left atrium, LV = left ventricle, RV = right ventricle. I also used red to represent oxygenated blood and blue to represent oxygen depleted blood. I represent the tricuspid and mitral valves with the valve graphics used in engineering diagrams. I drew the little curve on the Typical Heart drawing to show the vessels leaving the heart don’t intersect/mix as they cross one another.
Process Flow Diagram representations of the typical heart flow compared to a heart with d-TGA
It’s not an accurate anatomic representation with size and doesn’t depict all the ways the blood enters the heart or how the arteries go up and out of the heart. The vessels and all the valves aren’t even labeled, but I think it easily shows why TGA is such a critical heart defect. From my flow diagram, I think it’s clear the rest of the body can’t receive oxygen with d-TGA because blood from the lungs can’t be delivered to the rest of the body. As a healthcare professional or nursing student, I love the CDC and Cincinnati Children’s images to explain the heart and defects. However, as an engineer, I love the simplicity of my flow diagrams.
If you were a 5th grader, what graphics are easier to understand? What do you think about my depictions? For my next blog post, I’ll share the diagrams I made that show how a baby survives d-TGA until they receive surgery to switch the arteries and correct the flow to the lungs and body. Hint: Look at the ASD and PDA in the CDC graphic for the TGV heart.
I viewed this coaching/motivational video (https://www.youtube.com/watch?v=oDzfZOfNki4) by Duke Women’s Basketball’s Kara Lawson about how we need to “Handle Hard Better.” I share this post and video to motivate you as we reflect and head toward the weekend. Things get more challenging as we grow, develop, and learn. We become more skilled and adept at facing what’s in front of us. Again, things didn’t get easier – we just got better! We learned to handle hard better.
Another way to look at it: Walking was once difficult, but once I mastered that, I learned to use the stairs, jump, and eventually run. Once we become comfortable handling what we once thought was a challenge, it’s time to take on a new challenge to continue our growth and development. I didn’t even get “comfortable” with my old job or feel like I “mastered” it, yet I left and started a new one! I left my previous NICU (Level 2) to move to a higher acuity NICU (Level 4) because I knew I wanted to be able to handle more seriously ill patients.
I completed my first week with my preceptors at my new job, and it was a little overwhelming. Moving from a Level 2 NICU to a Level 4 NICU feels like a big jump. There’s so much to learn! In some ways, I feel like a new grad nurse all over again and have to familiarize myself with new equipment, processes, and diseases for my higher acuity patients. The video is a reminder to “handle hard better.” The way I handle hard better is to practice and expand my skills and to be willing to learn and open to coaching. I reflect on my performance and search for ways to improve. The way I handle hard is to do what I can to make myself better.
What does that look like for me? I am making report sheets or brains that work for me on my new unit and make me more efficient. I am learning about different disease processes by reading about them and watching YouTube videos. I am giving shift report even though I don’t feel like I’m ready because “doing” is better practice for me than “watching”. I’m learning the new charting system and what my new hospital requires for each shift. I’m learning about the workflow and general day-to-day schedule and expectations. I’m reflecting on my week by writing this post…and I’m giving myself grace that I’m still learning and will improve with more practice and time.
You may be hesitant to pursue a new job or career. You may be reluctant to go back to school. I am here to encourage you. I have met many second-career nurses, older students, and moms returning to college or joining nursing school since I became a nurse. My story is not unique. I share my life as a second-career nurse hoping to inspire others to pursue their dreams even when circumstances may seem hard. You can do it – you can “handle hard better”! Good luck on your journey!
NICU nurses in my hospital are responsible for putting IVs in our neonatal patients. We don’t have an IV team to do it for us, and often, our nurses are called to other units when other units have difficulty putting IVs in babies. Regardless, IV placement is an essential nursing skill, and putting IVs in infants is different than putting IVs in adults. For adults, I can usually see or palpate (feel) veins. For babies, it can be difficult to see veins, and I’ve never been able to palpate them. It had been a while since I placed an IV in a baby, so I asked and volunteered to do it for a colleague needing to replace an IV in her patient on my last shift.
I placed the IV in the patient, but not without almost giving myself a needle stick (I dropped the needle, and it rolled away from me before I could retract it) and having some blood splash from quickly releasing a used hub on a bedside table. I’ve never come close to giving myself a needle stick, nor have I created such a mess from attempting to place an IV. Senior nurses were present to help me hold down the baby and hold up a vein finder. I felt like I was fumbling through the process with an audience. I hadn’t worked with these nurses before to place an IV because I was still new to the night shift. And while I eventually got the IV in, I felt foolish with how long it took and how I splashed blood on the table. I’m embarrassed that this is the first impression I’ve given these nurses on my IV skills. In a way, however, it was confirmation that I needed the practice.
While I was placing the IV on my colleague’s patient, the IV on my patient stopped working and needed replacement. As soon as I placed the IV on my colleague’s patient, I hurried to my patient’s isolette. I attempted to put a new IV on my patient, got it during my second attempt (the vein blew during the first attempt), but then accidentally pulled out the catheter as I tried to remove the tape and Tegaderm to retape the IV. It had stopped flushing smoothly, and the other nurse and I thought we could retape it to prevent it from getting kinked or occluded. As a guideline, a different nurse should take over the IV placement after two unsuccessful attempts. I stopped with further IV attempts on my patient beyond my two tries but got the lesson to remove tape individually so as not to pull out an entire catheter when retaping. (I had initially tried pulling off the tape before the Tegaderm, but it was hard to separate it from the Tegaderm). My colleagues eventually got a new IV in my patient. I appreciate the teamwork, but I still feel embarrassed by how I kept “messing up.”
I wanted IV practice on my last shift, and the universe gave me multiple chances! As humbling as my previous shift was, I realize the only way to improve my nursing skills is with experience and practicing essential skills: I will be more consistent and successful at putting in IVs only by putting in more IVs. Luckily, NICU nurses support each other and help and assist one another during IV placements. However, there are times when the unit is busy, and nurses may not always be available to help each other. I want to feel more confident with doing IV placement alone. I will have to request to do IVs whenever there is a chance.
Sometimes, it feels weird to be older and yet so new in work experience. I must remind myself and give myself the grace that I am still relatively new to my profession. There’s a lot I’m still learning to do that senior nurses do effortlessly and automatically. And even the most experienced nurses make mistakes or are sometimes unable to get an IV placed on the first try. I can’t expect perfection, but I can at least aim for improvement.
When I had my baby, my husband and I struggled to feed our newborn. I wanted to breastfeed my baby exclusively, but she would not breastfeed well. Influenced by various sources and committed to breastfeeding, I refused to pump or bottle-feed my baby while in the hospital. My baby and I roomed in together while I tried to breastfeed. My husband recalls having to travel with my baby somewhere for light therapy. I vaguely remember this too, but I was tired, delirious from lack of sleep, and recovering from a C-section. I only remember sleeping while my husband and baby were out of the room. In retrospect, my baby most likely went to the NICU because she was jaundiced. She may have been there for only a few hours because I remember waking when my baby and husband returned from wherever they went. Thankfully, the hospital did not admit my baby to the NICU, and we could leave the hospital together. However, our struggles to feed our newborn continued when we got home. Looking back at our experience as new parents, I wish I had known some things about feeding our baby that I know now as an experienced mom and NICU nurse.
Photo by Helena Jankoviu010dovu00e1 Kovu00e1u010dovu00e1 on Pexels.com
Fed is Best
As a NICU nurse, I see term or late pre-term infants (born at 34-37 weeks gestation) who come to our NICU for hypoglycemia (low blood sugar) or hyperbilirubinemia (seen as jaundice/yellowish skin). Often, these term babies come to our unit because they are not eating well. For some babies, parents refuse to feed baby formula while postpartum, and the mom may not have established her breastmilk supply yet. This description reflected us as newborn parents and a likely reason why my baby needed phototherapy.
A build-up of bilirubin in a baby’s body can cause jaundice. Bilirubin is usually processed by the liver and leaves the body as waste. A newborn’s liver may not yet efficiently function, but the baby should be eating/drinking something to produce waste and encourage processing out bilirubin. A newborn baby drinking breastmilk or formula helps curtail jaundice. If a baby is not feeding well or is still jaundiced despite attempted feedings, however, hospitals can treat elevated bilirubin levels (hyperbilirubinemia) through light phototherapy.
Jaundice is normal in newborns, but the hospital monitors bilirubin levels and treats when levels rise above certain thresholds. If the baby’s bilirubin is too high, brain damage can occur. In our hospital, if a postpartum baby needs phototherapy, the baby is admitted to the NICU. Phototherapy in the NICU only happens after multiple attempted feedings and when bilirubin levels exceed treatment thresholds.
Frequent feedings are how parents can reduce bilirubin levels in otherwise healthy babies (and hopefully prevent hyperbilirubinemia that requires NICU care). However, frequent feedings can also help prevent another common condition in our NICU: hypoglycemia, or low blood sugar. If an otherwise healthy baby born to a non-diabetic mom takes enough breastmilk or formula, the baby can usually avoid hypoglycemia. However, if the baby is unable to feed adequately, the baby can develop low blood sugar.
Before a baby goes to the NICU for hypoglycemia treatment and monitoring, the mother and the postpartum staff will attempt to feed the baby. If the mother consents, the baby can be offered formula. If bottle-feeding is still insufficient, a sugar gel is given to the baby orally. The postpartum unit will attempt several feeding and sugar gel administrations before the baby goes to the NICU. If the NICU admits a baby for hypoglycemia, we will place an IV to deliver sugar to the baby as IV fluids. Once the sugar levels in the baby are sufficient, and the baby is drinking adequately, we can reduce the IV fluids and eventually remove IV fluids if the baby can orally consume the needed calories and fluids while maintaining healthy blood sugar and hydration. In the NICU, we try feeding our babies breastmilk if it’s available and not contraindicated (i.e., substance-abusing mother). If breastmilk is unavailable and we need to feed a baby orally, we will give provider-ordered formula to our babies.
For babies admitted for hyperbilirubinemia or hypoglycemia, I sometimes hear the baby barely drank anything because the baby was unable to breastfeed from a mom who wanted only to breastfeed exclusively. Before doctors send the baby to the NICU, the nurses can offer the baby formula if the mom consents or requests it. However, by this time, the baby may have worn themselves out or be too tired to drink from the bottle. It makes me and other NICU nurses wonder, “If the parent or nurses fed the baby from the bottle sooner, would the baby still need to go to the NICU? Is the mother promptly informed of her options if her milk supply hasn’t come in or the baby cannot latch or breastfeed?”
While I’m glad my husband got to go with my baby and accompany her for phototherapy, I would have preferred that my baby not leave my postpartum room at all for treatment or tests. To prevent my daughter from needing to leave our room, I would have pumped sooner to encourage my milk supply and produce milk that my husband or I could bottle-feed my baby. We did not learn until weeks later that my daughter was tongue- and lip-tied, which may have initially made it difficult for her to breastfeed. From my perspective, it’s better to feed a newborn some formula to keep the baby with mom and out of the NICU than to rely solely on breastmilk that may not be available yet or difficult for the baby to access.
Pumping is Okay
I was offered to pump in the hospital but refused, thinking I would breastfeed. My doula recommended not to pump until after the first month, so I tried holding off on pumping in an attempt to have my baby latch, help establish our breastfeeding rhythm, and set my breastmilk supply.
I didn’t want to feed her from a bottle because I didn’t want to cause nipple confusion and have my baby prefer the bottle over breastfeeding. When we got home, I thought I was doing okay breastfeeding, but when we brought our baby to her 1-week checkup, she wasn’t gaining enough weight. We brought her to her 2-week checkup, and her pediatrician still didn’t think she was gaining enough. My daughter fell in the 2nd percentile on the growth chart. (I did not discover until months later that my husband and his siblings were so small as newborns they were not even on the growth chart). We were strongly encouraged to start bottle feeding her formula.
Wrought with guilt, we decided to feed her some formula, and I began to pump. By this time, I had developed mastitis (Mastitis is a painful infection in the breast caused by bacteria introduced by breastfeeding. It also caused me to have body aches, a high fever, and chills. Imagine dealing with this while trying to care for a newborn!) My supply was woefully insufficient, and most of my daughter’s caloric intake was formula once I started to pump while battling mastitis.
Formula is Okay
It is okay to use formula if you are not producing breast milk or enough breast milk/colostrum to feed your baby. I wanted to exclusively breastfeed because I learned about the benefits of breastfeeding and how it’s the best, natural, and easiest way to feed my baby. It’s great for baby bonding and helps provide passive immunity to the baby. However, I got mastitis TWICE within the first month or so of my daughter’s life. We also learned my daughter was tongue-tied, making it difficult for my daughter to breastfeed. Not until later did I meet other mothers who breastfed AND bottle-fed their babies or moms who exclusively pumped. (Moms who exclusively pump only feed their babies breastmilk from a bottle). Had I not been so attached to exclusively breastfeeding, I could have adapted and explored these other options earlier as a new parent.
Do What’s Best for You and Your Family
Aside from taking antibiotics, the way to clear a mastitis infection from the breast is by breastfeeding or pumping. My daughter preferred the bottle by this time, so I relied on pumping to clear my infection. Pumping (and antibiotics) eventually relieved the pain and released the mastitis in my breasts, but the repeated infections impacted my supply. Encouraged by my doula, I remember three days where I spent about 9 hours pumping (diligently pumping 45 minutes every 2 hours, per her recommendation) only to produce about 1 ounce of breastmilk daily. I was so exhausted and upset by the results of my efforts. I also felt cut off from my daughter while I pumped (Because I couldn’t figure out how to safely hold her with all the pumping tubes hanging from my body, my husband or parents would take her while I pumped). After the three days dedicated to pumping round-the-clock, I decided it was not worth it to continue to pump. It was more important for me to be with my baby than to try giving her my pumped breastmilk.
I still held out hope for breastfeeding. Once my infection cleared, I tried to breastfeed my daughter using an SNS (supplemental nursing system – a tube placed on the breast but connected to a bottle to measure and ensure the baby has adequate intake). She was already used to the bottle nipple and did not take to the SNS. I attempted multiple times, but she would refuse to feed through the SNS, and I would end up with formula spilling all over my chest.
I share a bit of my breastfeeding journey to emphasize that there are many ways to feed and nourish a baby. In the end, so long as the baby is healthy and safe, parents decide what works best for them and their family. The caregivers’ mental health and well-being are as important as the baby’s. The way you choose to care for your baby may not resemble how other families do things, and that’s okay. I was ashamed for not breastfeeding my daughter for as long and in the way I hoped, but I felt my attachment to breastfeeding distanced my baby from me and caused so much anxiety and distress. Parents should not be ashamed of doing what is best for them and their families.
In the NICU, I meet moms who feel nervous they cannot directly breastfeed, yet they can pump and produce enough breastmilk to meet their baby’s needs. I meet parents who are ashamed they don’t have a separate nursery for their baby. We live in Los Angeles – not every family can afford to pay for a home with different bedrooms for each of their children! Many of our parents rely on WIC because they can’t afford to purchase formula. Getting formula from WIC is better than diluting formula or not feeding the baby enough nutritious calories. I try to assure the parents I see they can do what works for their family – it doesn’t need to match other families.
I felt defeated when I finally gave up pumping and breastfeeding. I wish I gave myself a little grace as a newborn mom and wasn’t so hard on myself. I felt so much grief over my inability to mother and feed my child as I thought I should that it made me feel inadequate as a mom. I was separated from my baby while I pumped, trying to salvage any breastmilk I had. I cried every day when I was pumping or trying to breastfeed. Ultimately, I fed my baby adequately, thanks to formula, and my child is now a healthy school-age girl. She still falls on the low end of the growth chart, but her father and I are not tall, so my daughter’s standard is the tenth percentile or less.
As I reflect on my experience as a new mom, I hope to impart grace and support to other new parents now that I’m a NICU nurse. If a caregiver is feeding their baby adequately, caring for and bonding with them, and keeping them safe, I want them to know they are doing a great job! I also want them to know it’s okay to make adjustments as needed or change their minds about how they want to do things. Parents can adapt their plans according to the family’s needs.
I originally wrote this post to give insight on how to lower the likelihood of hyperbilirubinemia or hypoglycemia (and admission to the NICU) through frequent feedings. If this information helps reduce NICU admissions and prolong in-room bonding between caregiver and baby, I would be ecstatic. Ultimately, I hope this post reassures parents (and serves as a reminder to myself) that there are many ways to care for a baby. There are no perfect parents; there are no perfect children. We’re just doing our best with the information and resources we have. Good luck to you on your journey!
Nursing requires emotional regulation in a way that engineering never demanded. If an engineering project experienced delays in my former consumer products and manufacturing career, I could have a lot of anguish, and managers may be upset. Still, such delays generally wouldn’t impact someone’s activities of daily living, quality of life, or health and well-being. There are a lot of passionate reactions when a family member expects to take their loved one home from the hospital but cannot for whatever reason. When there are unexpected treatments, tests, or further monitoring patients must undergo, people get frustrated, particularly when they feel their health issues are unresolved or worsening. The family members or patients express their frustrations with their nurses. I try my best that my patients or families feel heard or understood, but sometimes, a healthcare worker’s efforts are not enough or provide little comfort.
I’ve witnessed codes ending in unexpected deaths, and I still have to be present and care for other patients while surviving family members grieve. I’ve dealt with emotionally unstable, angry, or stressed-out patients and family members. Patients have attempted to hit me or have cussed me out. I don’t take it personally, but I sometimes fear for my safety. I feel like these instances of feeling unsafe have drastically dropped since I started working in the NICU. However, I still float to the PICU or Pediatric units. During my orientation in the Pediatric ward, a 4-year-old patient tried to bite me when another nurse and I tried to change his ostomy bag. Shortly after my cross-training to the Pediatric unit, I had a Pediatric teenage patient attack her sitter. These instances are further reminders of why I chose to work in the NICU over other units. But witnessing these events made me realize that it’s not helpful to react emotionally to dysregulated patients. I’ve seen healthcare workers respond angrily, and it does nothing to help de-escalate situations.
Aside from navigating emotional pitfalls with my patients or their family members, I’ve had to figure out how to deal with specific staff and co-workers. I have had to learn who and how to ask for help or get people to do their jobs so I can do mine to ensure my patients are getting appropriate care. Certified Nurse Assistants (CNAs) typically support registered nurses (RNs) by performing activities of daily living for a patient, taking vital signs, or acting as sitters. RNs are responsible for ensuring the CNAs work is documented and must oversee and support the CNAs work. As a new grad, I’ve had to correct a grumpy CNA about proper hand hygiene or continuously remind a CNA to document their work in the patient’s chart. I like that I don’t have to worry about this in the NICU. In the NICU, we have no CNAs. I appreciate this versus negotiating or constantly confronting an uncooperative CNA to do work or documentation. Don’t get me wrong, just as with any role (Charge nurse, RN, Doctor, etc.), some CNAs are incredible, but some are not. I like having one less variable to deal with during my shifts.
I think it’s good to get a sense of your limitations and your ability to regulate yourself emotionally. I love babies and children, but I chose to work in NICU and not focus on Pediatrics for the genuine concern of being unable to regulate myself emotionally with pediatric patients. Anyone I’ve personally known who’s had a baby in the NICU has had their child leave and carry out healthy lives. My daughter will never be at risk of being in the NICU – she’s way past that stage. However, when I find myself in pediatrics, I see patients there that could be my child – some are there due to some freak accident or unknown illness. One of the most recent times I was in the PICU, a toddler or preschooler was getting intubated on the other side of the unit – I started to tear up as the patient was wailing and crying, “Mama” while their mother held them to prepare for the procedure. I was grateful this wasn’t my patient and tried to distract myself from their cries and their distressed parents by focusing on my patient.
It’s good to see parents involved with their children’s care, but other pediatric patients are there because of abuse by family members and adults. Some of the children’s social situations are sad. I can’t dwell too much on this as I care for my patients, and I try to give the child the best care I can while they’re my patient. I try to develop a trusting relationship with patients (or family members) by promptly communicating with them and responding to their needs. For abused patients, I sometimes tell myself, “This child’s life before they arrived at the hospital may not have been so great, but I can care for them and provide some stability and safety while they’re under my care.”
Complex social problems can also occur with our neonatal patients. I see my fair share of neonatal patients in our NICU because of maternal drug use – some mothers are remorseful of their actions and are in rehab programs, while others have no desire to quit using. Sometimes it’s hard for the moms to see their inconsolable babies withdrawing and know their baby is struggling because of their drug use during pregnancy. Some babies go home with their families despite drug use, and others do not. Either way, as a nurse, I try to support the caregivers taking the babies home and educate them on how to care for their babies. I’m responsible for the care of my patient while they’re in the hospital, but I also want to support their caregivers and give them confidence in being able to care for their babies (or children) when they leave.
I’ve never had a job that demanded so much of me every day. Nursing can be mentally, physically, and emotionally draining. Until I became a nurse, I don’t think I realized the impact nursing has on a person holistically. I like helping people, I like that I can do that as my job, and I want to be able to do that for a long time. I always heard about the nursing shortage but never really considered that what was contributing to that was nursing burnout and nurses leaving the profession until I started pursuing nursing as a second career. It’s essential to be aware of the typical challenges nurses face to determine how you will guard yourself and strategies for longevity in the profession. I hope this series of posts helps provide insight into what it’s like as a novice nurse and some of the things I do to keep myself connected to the things I love about Nursing. Good luck! If any other nurses out there have other advice to share, I’d love to hear it!
Nursing can be very physically demanding – many patients require assistance turning, lifting, or moving body parts or equipment. I attended a safe-patient handling workshop offered by Daniel Tiano, a physical therapist whose goal is to “enable healthcare workers to fulfill their vocation without being held back by pain and injuries.” He compared nurses to endurance athletes, constantly lifting, turning, pushing, and pulling hundreds of pounds over a 12-hour shift. While I work primarily with neonates now that I’m a NICU nurse, I can still get floated to pediatric or post-partum wards and handle heavy patients. Pediatric patients are not always light, easy-to-handle patients. I’ve cared for adolescents over 80 kg and adults (18-25 years old) in pediatric units.
I must handle my patients carefully to avoid ergonomic injuries, even with babies. [Tips: Raise and lower beds or cribs to prevent back strain! Get assistance when lifting patients, and use lifting tools!] I know from experience that I can hurt more than just my back when caring for babies. As a new mom, I developed tendonitis because I held my newborn with my wrists bent. My baby wasn’t heavy to carry, but I still injured myself. My tendonitis pain went away after treatment and physical therapy. I’m more conscious now and deliberate about holding babies with my wrists straight!
Aside from modifying my behaviors to make sure I don’t cause myself injury, I have to be alert to other people’s behaviors. Patients (or their families) can have behavioral issues and be violent. As a nurse, I have to be careful that certain patients do not harm my co-workers or myself. Unfortunately, one of my teenage patients attacked her sitter/nursing assistant during one of my recent shifts. A nurse must continually assess their patient and environment to keep not only their patients safe but themselves safe, too.
Some patients (or their visitors) have mental health or drug use issues that make them unstable. Other patients may have temporary delirium due to infection or illness, causing verbally or physically abusive behavior that they usually would not have. I have cared for patients that have tried to hit, kick, or bite me or have yelled, cursed at me, and called me names. This danger doesn’t exist only in adult units. My NICU colleague had a teenage patient throw a monitor at her when she floated to the Pediatric unit. Honestly, I have more physical and personal safety considerations each day in my nursing job than in my previous career. I think that says a lot considering I was a certified Hazardous Waste Operator (HAZWOP) who periodically cleaned up hazardous material spills while I was an engineer!
Anyone working in hospitality or customer service is probably used to dealing with all kinds of people. My former preceptor used to be a restaurant server, and she said it helped prepare her for dealing with all types of patients in nursing. However, nursing is very different from what I was used to in my prior career. I never felt unsafe or in danger of other people when I was at work. I worked in a secured facility for over 18 years – people from the street couldn’t walk in, and we didn’t serve the public at my site.
In contrast, when you work in a hospital, you see all kinds of people, and often, people are emotional, in unresolved suffering and pain, or the most unstable they have ever been. It’s a ripe environment for people to lash out, potentially violently. Healthcare workers encounter violent behavior so often that facilities often require their employees to get certification in Management of Assaultive Behavior (MAB). As a NICU nurse, I haven’t encountered violent parents (hopefully, this NEVER happens). Still, I have observed emotional and angry parents with whom I must be careful and anticipate volatile behavior.
Bedside nursing is a physically demanding job. A nurse should exercise, eat energizing foods, and get enough rest to stay healthy and physically well. That applies to ANYONE. However, a nurse must also act like an endurance athlete and self-defense master. Aside from the typical actions to stay physically well or safe, nurses must be aware of body mechanics and constantly read behavioral cues from others. Thankfully, I’ve been safe and injury-free so far, but I’m still trying to figure out how to be more healthy, so I have the stamina and longevity to be a bedside nurse. I’m on a journey and will continue to share. Stay tuned for the next part of my novice nurse series, where I discuss handling my emotions as a new nurse.
Welcome to Part 2 from a series of posts about what I learned as a new nurse and the demands of nursing.
It took a while for me to transition into nursing and adjust to my newfound career and job expectations. After working over eighteen years with the same company in a consumer products/manufacturing setting, I grew accustomed to a certain rhythm in my job as an engineer/scientist. I was a salaried employee in my previous career as an engineer and never needed to clock in or out. Some days could be stressful when I was an engineer, but mainly, I could set my day-to-day schedule. I didn’t have a required shift to start by six or seven each morning. I would have project deadlines to meet, but they didn’t necessarily dictate what I did every hour of each workday. I could go to the bathroom when I pleased or schedule my lunch to eat with friends. I had a lunch squad. If I was behind with my schedule, I could stay late. When I wasn’t periodically supporting shift work in the manufacturing plant, I started my days mostly between 8a and 9a and ended around 6:30p – 8p. Each workday as an engineer, I did not have to consider getting my work assignments from a prior shift, passing work along, getting and giving shift reports, nor did I need someone to take over my work during my bathroom or meal breaks.
I work in a hospital now, so my shifts as a nurse are dictated each day. Sometimes, there’s no time for me to pee, drink, or eat as a nurse. I eventually get to do these things, but not necessarily when I want. Hourly tasks (assessments, med passes, labs, and patient ADLs) dictate each workday. My patients and their needs and orders direct my priorities for each day. I have no lunch squad. I can’t go on meal breaks with my co-workers because they need to cover my patients when I go on break. Sometimes, the charge nurse makes me go on my snack and meal breaks when I am not ready to ensure proper coverage. If I think things are a little slow or I have some downtime, that’s when admission or some unexpected event likely occurs. (This is why you never use the “Q” word – “quiet” – to describe the environment or shift around nurses – you jinx them into having a chaotic shift later).
I’ve learned it’s better to accomplish tasks early rather than on-time because one emergency or tricky issue can cause a delay to an entire planned schedule that was once “on time.” For example, when I was in Med-Surge, I had to do unscheduled sacral wound dressing changes for an incontinent, primarily immobile, continuously stooling patient. Each time I’d get help to turn and lift the patient, clean them, replace their diaper and linens, and do the dressing change, the patient would soil themselves and their new dressing. These kinds of time-consuming, unplanned activities aren’t limited to adult patients. More recently, when I was floating to our Pediatric ward, an ostomy bag for a hyperactive non-compliant preschool patient kept leaking and needed continual replacement. The patient would purposely peel off their ostomy bag and then resist having it changed. Even though the patient was a preschooler, one person needed to help hold down the patient and keep the patient still to allow another person to replace the ostomy bag. Such unplanned activities take time and can cause delays in other scheduled tasks. I was used to addressing shifting priorities and non-compliances as an engineer, but I never had hourly assignments that could jeopardize people’s health if completed late or improperly.
It was hard for me to account for unexpected, unscheduled tasks as a new grad nurse. It can still be frustrating, but I feel I’m not as flustered, and it doesn’t have to thwart the rest of my day. I have learned to do things as early as possible to leave room for the unexpected. My last NICU preceptor also encouraged me to accomplish tasks as soon as possible to be available to help other nurses. Thankfully, nurses in my department jump in and help one another. However, my preceptor warned they may not be as willing to help me if I’m always busy and unable to help them when they need assistance. As I shared, some activities require coordination of availabilities and assistance from other nurses or nursing attendants. I want to be a team player that others can count on for help. Accomplishing tasks early not only makes my life easier, preparing for the unexpected, but it also allows me to help others with their patients or tasks. However, even when I am able and want to accomplish tasks before they are due, I can’t always do this. For instance, I must still ensure meds are given in an appropriate timeframe and not too early to avoid overdosing patients.
Critical thinking and mental alertness cannot be lax as a nurse. (This is also how I justify my caffeine intake). At best, a nurse’s mistakes may cause inconvenience; at worst, permanent injury or death. Any mistake I made as a process engineer could cost hundreds of thousands of dollars, but it would never cause bodily harm or death. There was a lot of oversight, approvals, and quality control with my work as an engineer. I feel like there are fewer checks and balances for nurses for the tasks they complete.
A nurse performs activities based on orders and nursing judgment. There is no constant oversight or approval process when a nurse administers many medications or completes orders. In contrast to process engineering mistakes, a medication error can kill. Not reporting critical labs or assessment findings can cause delays in treatment or interventions. I can’t consult with a weekly project team if I’m behind on my nursing tasks. I have to figure out who to ask for help to catch up with my work or quickly judge if it’s acceptable to be late, reschedule a task, or if I need to escalate issues. Aside from impacting patient care, nursing mistakes and errors can threaten nursing licenses. When I made mistakes as an engineer, I may have received criticism and a poor performance rating, but I never worried that I’d lose my ability to work as an engineer.
Given the pressure and expectations of nursing, my anxiety levels are higher than when I was an engineer or scientist. Some stress is healthy and helps keep my patients and me safe by forcing me to focus, ask for help, or take time with unfamiliar tasks or medications. However, until I became a nurse, I never realized how common it was for nurses to have or develop hypertension, anxiety, or depression. I’ve heeded the warnings of veteran nurses who advised me not to take overtime if I don’t need it, lest I end up with hypertension, like them.
I did not switch careers only to develop medical issues from my job. It’s one thing to manage high blood pressure, generalized anxiety disorder, post-traumatic stress disorder, or major depressive disorder, but it’s another to develop these conditions because of one’s job. Nurses need healthy coping mechanisms, as stated in my last post. I respect that sometimes it’s not enough to have healthy coping mechanisms or rely on comfort wisdom; various conditions require medication. However, Kelsey Rowell, RN Career Coach and founder of @wholelifenurse shared recently on her Instagram, “If your nursing job is requiring you to go on or increase your medication to support your mental health, that is your sign to find a new job, take a break, or do something else.” I wholeheartedly agree with her statement. Since I’ve switched to NICU nursing, my anxiety levels are lower than when I was a Float nurse for adults. Part of that may be due to having more experience or not working the night shift for the moment, but I think my decreased stress is also because NICU nursing is a better fit for me. There are so many opportunities within nursing that if a particular job is causing medical or mental health issues, try changing your nursing job!
What’s also relieved some of the new grad anxiety and pressure is recognizing that nursing is a practice. With more time and experience, I can improve my nursing practice. With more exposure to various units or patients, I learn what I like or dislike about specific nursing roles and can set my boundaries and determine my career goals. With more experience, certain medications or typical treatments will become more familiar. I will more easily recognize the signs or symptoms of conditions I regularly encounter. I can determine which skills are essential to master for various units or roles. (Tip: time management is a critical skill, no matter where you work as a nurse)
I have accepted that I’m imperfect and will make mistakes. Even veteran nurses make mistakes. When making mistakes, it’s essential to be transparent to a charge nurse or provider to correct errors or get help and alignment to move forward. Mistakes can serve as lessons. I’ve made mistakes in my engineering and nursing career that I know I will not make again because I never want to feel as compromised or ashamed as when I made the mistakes.
I want to prevent making mistakes that injure or permanently damage patients. One of my NICU preceptors said to accept that I will make mistakes but to spend time making sure I don’t make medication errors. If I spend more time evaluating an unfamiliar medication, dosage, or route, I accept that I will appear slow because of my uncertainty. I will ask for help or clarification. I will move more slowly and risk falling behind on my tasks rather than harmfully administering medication.
ANY new job or career produces increased stress and mental challenges. Some level of discomfort is healthy and helps us to learn and grow. It takes time to learn the protocols or processes of a new organization or unit. No one is perfect, and we all make mistakes. Sometimes, you understand how to be more efficient or effective by making mistakes or witnessing them. It takes time to learn who to ask for help, what requires escalation, and the chain of command. Over time, we know the methods of communication our co-workers, bosses, or patients/clients prefer. Skills cannot improve until you’ve practiced and done them many times. Understanding all this and having the mindset that I’m still learning (“I’m developing, not deficient!“) has helped relieve some of my new grad/novice nurse anxiety.
I hope this post gave some insight into the mental challenges of nursing and the mindset one has to have to thrive as a novice nurse. If you have any advice on how to handle the pressures of nursing or the mental challenges, please share! Thanks for reading! My next posts in this novice nurse series will discuss how I address the physical and emotional challenges of being a nurse.
Aside from an abundance of job opportunities, one of the things that attracted me to nursing was the schedule. Typically, nurses who work 12-hour shifts in hospitals work only three days a week. It seemed ideal to have four days off weekly to have more time with my family. I felt I could manage to work obligatory weekends and holidays when I already had worked weekends and holidays in my previous career as an engineer. I was used to working 12+ hour days as an engineer and would periodically do shift work, working overnight. When I wasn’t doing shift work, I would work weekdays, but work would follow me home, or I’d be on-call 24/7. I could work long hours and focus my energy on launching a product, completing a project, or passing an audit. I learned how to be a hard worker and resilient to get through challenging work assignments or situations in my previous life as a chemical engineer. However, I don’t think I’ve ever had to work as hard as an engineer on a day-to-day basis as I do each shift as a nurse.
Nursing takes a lot out of me. At the end of a shift, it’s common to be mentally, physically, and emotionally drained. Maybe it’s because I’m older, but I genuinely feel the work and energy required for nursing does not compare to when I was an engineer.
I came across a Business Insider article citing well-paying low-stress jobs. Nursing is nowhere on that list. Is it ironic that chemical engineers top the list at number 2? I chose to leave a relatively low-stress job and transitioned into one of the most stressful professions. Additionally, I became a nurse in the middle of a frickin’ pandemic!
While I do not have to work four days out of a week, it takes a lot more time to recover my energy from working nursing shifts than when I was an engineer. Also, when I worked night shifts as a nurse, the entire next day/night off would be a complete wash – I’d spend my day off napping, recuperating, and re-adjusting to my family’s schedule while still feeling like a zombie. Sometimes I’d need two days before I could feel fully functional and alert during the day and meaningfully interact with my family and friends. Just as I’d start to adjust, I’d have to work a block of night shifts and begin my cycle over again. I’m currently working day shifts, but I sometimes still need a whole day to recuperate after working. I have to be aware of my body’s needs and rest on days off, even when I have every urge to pack my schedule with outings and activities. I want to take advantage of my extra days off but recognize I need to spend some of that time relaxing or recovering. I might have the time to do something, but do I have the energy?
Admittedly, I never worried about having the energy to do something when I was younger. I kept a packed schedule – even on weeknights after work. (I think I also was more tolerant of toxic relationships and hostile work environments and did not realize how draining those could be). Maybe I seemingly had more energy because I was single and didn’t have family committments or time to devote to a spouse or children. It’s possible I had way more energy – or I just felt that way – because I could sleep in when I needed. (I’m a parent to a kindergartener; it’s been years since I slept in late). Now that I’m older, not getting enough rest impacts me more. Or maybe I’m simply more aware of my body’s needs than when I was younger.
Being self-aware helps me determine how to restore my energy. For instance, I’m an extrovert and need to connect and interact with people for my well-being. My introverted husband needs the opposite. Earlier in our relationship, I realized that going from party to party would make him miserable, while I would be happy and energized from the social interactions. As a result, I’m more selective with our social commitments.
When figuring out what to do on my days off, an essential question is: “Do I have the energy?” If not, what do I need to do to regain my energy? One of the ways I recover is by spending time with friends. I try to include social activities on my weekly calendar, even if it’s over Zoom. I did this throughout my pre-requisites and nursing school as well. Because I’m an extrovert, social interactions are crucial to maintaining my sanity and happiness. I felt dates with my friends or family were especially important during nursing school when my schedule would be packed with classes, clinicals, and studying. These dates could be simple lunch outings, coffee/tea, seeing a movie with my husband, or Zoom calls (critically needed during pandemic surges and lockdowns). I needed to make sure I had something social in my weekly schedule to feel balanced. I mentioned it before in other posts, but it helps to know what brings you comfort. I didn’t learn this in school – time and life experience have taught me “comfort wisdom” (a la Brene Brown). Have you developed healthy coping mechanisms? What do you enjoy as stress relief? Nursing school is stressful, but working as a nurse is even more so. Build a foundation of healthy responses to stress before or during nursing school to combat the stress and anxiety that frequently accompanies working nurses.
While being a nurse can be draining at times, I honestly love it. I can feel tired and overwhelmed, but there are moments where I’m interacting with patients and at peace and content with making a difference in someone’s life. People going into nursing naturally want to help people, but they need to understand how demanding nursing can be. Until I started working as a nurse, I don’t think I realized just how stressful a job nursing could be. Prospective and new nurses need to understand what they can do to protect and restore themselves to continue in this rewarding profession. I have so much to share about this topic that I thought I would make this and the next several posts about addressing the mental, physical, and emotional demands of being a nurse. I want to candidly share what it’s like for me and what I do to try and guard myself against being drained or burnt out. And yes, unfortunately, burnout can happen to early-career nurses, too, not just veteran nurses.
I hope what I’ve shared – and what I plan to share – is helpful and provides some honest insight – see you in my next post on this series!