As a bedside nurse, part of my job is to perform patient/family education. It is honestly one of the things I love to do. Since I’m in the NICU, I do most of my teaching to parents and families instead of to my neonatal patients. I can teach parents about how to care for their baby with lessons on feeding, diapering, or bathing, but I can also reinforce their understanding of their child’s diagnosis or medical condition.
At my Level IV NICU, we tend to see a lot of cardiac patients and babies born with congenital heart defects (CHD). Some of these conditions are rare and not easy to understand; even more difficult to understand without knowledge of how a normal heart works. Personally, I never knew or understood blood flow through the heart until I took anatomy and physiology. Not all our parents or caregivers have had anatomy and physiology. So how do I explain what’s going on with their baby?
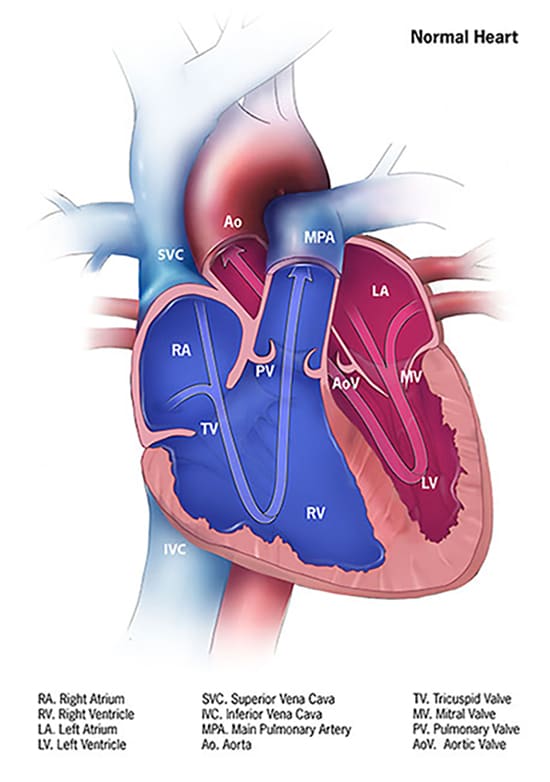
There are reputable websites I can refer to that have pictures to better understand CHD – I think they’re great for healthcare professionals and nursing students as well. One of them is the Centers for Disease Control and Prevention https://www.cdc.gov/ncbddd/heartdefects/index.html.
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
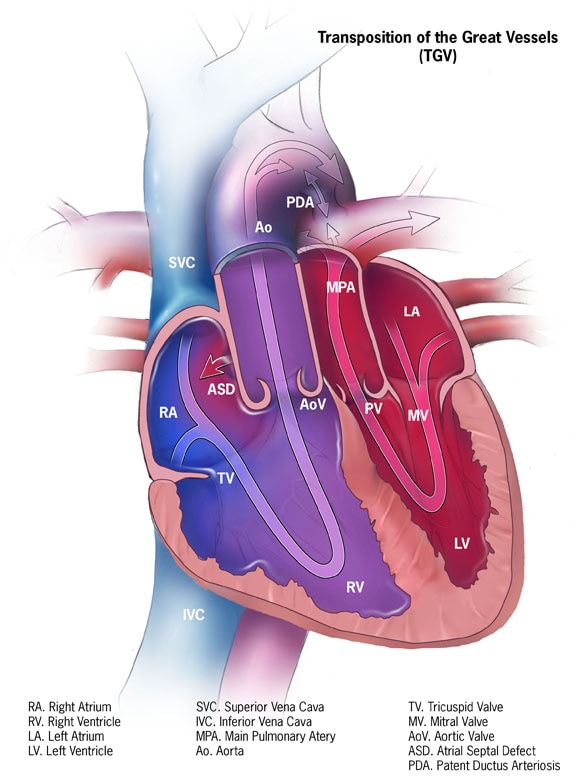
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
Another website that’s a great resource for CHDs is Cincinnati Children’s https://www.cincinnatichildrens.org/service/c/cardiothoracic-surgery. Cincinnati Children’s even offers animated heart videos to illustrate various heart conditions. While I love and recommend these resources, I’ve been wondering how I could further simplify patient teaching. In nursing school, I was taught to conduct patient teachings at the 5th grade level. Healthcare professionals should simplify teaching to their patients and patients’ families and use words such that a 5th grader could understand.
Recently, I’ve been thinking about teaching for a family who had a baby come to our hospital with a rare congenital heart defect, Transposition of the Great Arteries (TGA, or d-TGA). They seemed hesitant in explaining their child’s condition. They held up their hands and shared their baby’s arteries need to be like this (as they held their hands up, crossed like an ‘X’) but that their baby’s arteries are like this (as they held their hands parallel) to each other. They were not wrong in their explanation, but I wondered if they understood why it needed to be “crossed”. I felt like a process diagram could have been helpful.
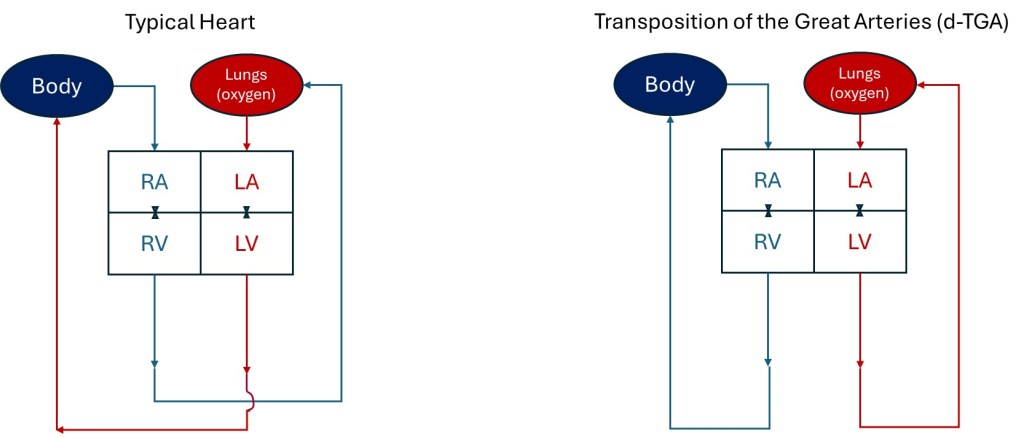
As a former engineer, I used to make flow charts in either designing or explaining existing manufacturing processes. I really wanted to simplify the explanation of blood flow to /from the heart with a process diagram. I drew it out when I got home and then tried to replicate what I drew on the computer. Below are the process flow diagrams I designed, using the same abbreviations as the CDC used to describe parts of the heart in their diagrams: RA = right atrium, LA = left atrium, LV = left ventricle, RV = right ventricle. I also used red to represent oxygenated blood and blue to represent oxygen depleted blood. I represent the tricuspid and mitral valves with the valve graphics used in engineering diagrams. I drew the little curve on the Typical Heart drawing to show the vessels leaving the heart don’t intersect/mix as they cross one another.
Process Flow Diagram representations of the typical heart flow compared to a heart with d-TGA
It’s not an accurate anatomic representation with size and doesn’t depict all the ways the blood enters the heart or how the arteries go up and out of the heart. The vessels and all the valves aren’t even labeled, but I think it easily shows why TGA is such a critical heart defect. From my flow diagram, I think it’s clear the rest of the body can’t receive oxygen with d-TGA because blood from the lungs can’t be delivered to the rest of the body. As a healthcare professional or nursing student, I love the CDC and Cincinnati Children’s images to explain the heart and defects. However, as an engineer, I love the simplicity of my flow diagrams.
If you were a 5th grader, what graphics are easier to understand? What do you think about my depictions? For my next blog post, I’ll share the diagrams I made that show how a baby survives d-TGA until they receive surgery to switch the arteries and correct the flow to the lungs and body. Hint: Look at the ASD and PDA in the CDC graphic for the TGV heart.
Welcome to Part 2 from a series of posts about what I learned as a new nurse and the demands of nursing.
It took a while for me to transition into nursing and adjust to my newfound career and job expectations. After working over eighteen years with the same company in a consumer products/manufacturing setting, I grew accustomed to a certain rhythm in my job as an engineer/scientist. I was a salaried employee in my previous career as an engineer and never needed to clock in or out. Some days could be stressful when I was an engineer, but mainly, I could set my day-to-day schedule. I didn’t have a required shift to start by six or seven each morning. I would have project deadlines to meet, but they didn’t necessarily dictate what I did every hour of each workday. I could go to the bathroom when I pleased or schedule my lunch to eat with friends. I had a lunch squad. If I was behind with my schedule, I could stay late. When I wasn’t periodically supporting shift work in the manufacturing plant, I started my days mostly between 8a and 9a and ended around 6:30p – 8p. Each workday as an engineer, I did not have to consider getting my work assignments from a prior shift, passing work along, getting and giving shift reports, nor did I need someone to take over my work during my bathroom or meal breaks.
I work in a hospital now, so my shifts as a nurse are dictated each day. Sometimes, there’s no time for me to pee, drink, or eat as a nurse. I eventually get to do these things, but not necessarily when I want. Hourly tasks (assessments, med passes, labs, and patient ADLs) dictate each workday. My patients and their needs and orders direct my priorities for each day. I have no lunch squad. I can’t go on meal breaks with my co-workers because they need to cover my patients when I go on break. Sometimes, the charge nurse makes me go on my snack and meal breaks when I am not ready to ensure proper coverage. If I think things are a little slow or I have some downtime, that’s when admission or some unexpected event likely occurs. (This is why you never use the “Q” word – “quiet” – to describe the environment or shift around nurses – you jinx them into having a chaotic shift later).
I’ve learned it’s better to accomplish tasks early rather than on-time because one emergency or tricky issue can cause a delay to an entire planned schedule that was once “on time.” For example, when I was in Med-Surge, I had to do unscheduled sacral wound dressing changes for an incontinent, primarily immobile, continuously stooling patient. Each time I’d get help to turn and lift the patient, clean them, replace their diaper and linens, and do the dressing change, the patient would soil themselves and their new dressing. These kinds of time-consuming, unplanned activities aren’t limited to adult patients. More recently, when I was floating to our Pediatric ward, an ostomy bag for a hyperactive non-compliant preschool patient kept leaking and needed continual replacement. The patient would purposely peel off their ostomy bag and then resist having it changed. Even though the patient was a preschooler, one person needed to help hold down the patient and keep the patient still to allow another person to replace the ostomy bag. Such unplanned activities take time and can cause delays in other scheduled tasks. I was used to addressing shifting priorities and non-compliances as an engineer, but I never had hourly assignments that could jeopardize people’s health if completed late or improperly.
It was hard for me to account for unexpected, unscheduled tasks as a new grad nurse. It can still be frustrating, but I feel I’m not as flustered, and it doesn’t have to thwart the rest of my day. I have learned to do things as early as possible to leave room for the unexpected. My last NICU preceptor also encouraged me to accomplish tasks as soon as possible to be available to help other nurses. Thankfully, nurses in my department jump in and help one another. However, my preceptor warned they may not be as willing to help me if I’m always busy and unable to help them when they need assistance. As I shared, some activities require coordination of availabilities and assistance from other nurses or nursing attendants. I want to be a team player that others can count on for help. Accomplishing tasks early not only makes my life easier, preparing for the unexpected, but it also allows me to help others with their patients or tasks. However, even when I am able and want to accomplish tasks before they are due, I can’t always do this. For instance, I must still ensure meds are given in an appropriate timeframe and not too early to avoid overdosing patients.
Critical thinking and mental alertness cannot be lax as a nurse. (This is also how I justify my caffeine intake). At best, a nurse’s mistakes may cause inconvenience; at worst, permanent injury or death. Any mistake I made as a process engineer could cost hundreds of thousands of dollars, but it would never cause bodily harm or death. There was a lot of oversight, approvals, and quality control with my work as an engineer. I feel like there are fewer checks and balances for nurses for the tasks they complete.
A nurse performs activities based on orders and nursing judgment. There is no constant oversight or approval process when a nurse administers many medications or completes orders. In contrast to process engineering mistakes, a medication error can kill. Not reporting critical labs or assessment findings can cause delays in treatment or interventions. I can’t consult with a weekly project team if I’m behind on my nursing tasks. I have to figure out who to ask for help to catch up with my work or quickly judge if it’s acceptable to be late, reschedule a task, or if I need to escalate issues. Aside from impacting patient care, nursing mistakes and errors can threaten nursing licenses. When I made mistakes as an engineer, I may have received criticism and a poor performance rating, but I never worried that I’d lose my ability to work as an engineer.
Given the pressure and expectations of nursing, my anxiety levels are higher than when I was an engineer or scientist. Some stress is healthy and helps keep my patients and me safe by forcing me to focus, ask for help, or take time with unfamiliar tasks or medications. However, until I became a nurse, I never realized how common it was for nurses to have or develop hypertension, anxiety, or depression. I’ve heeded the warnings of veteran nurses who advised me not to take overtime if I don’t need it, lest I end up with hypertension, like them.
I did not switch careers only to develop medical issues from my job. It’s one thing to manage high blood pressure, generalized anxiety disorder, post-traumatic stress disorder, or major depressive disorder, but it’s another to develop these conditions because of one’s job. Nurses need healthy coping mechanisms, as stated in my last post. I respect that sometimes it’s not enough to have healthy coping mechanisms or rely on comfort wisdom; various conditions require medication. However, Kelsey Rowell, RN Career Coach and founder of @wholelifenurse shared recently on her Instagram, “If your nursing job is requiring you to go on or increase your medication to support your mental health, that is your sign to find a new job, take a break, or do something else.” I wholeheartedly agree with her statement. Since I’ve switched to NICU nursing, my anxiety levels are lower than when I was a Float nurse for adults. Part of that may be due to having more experience or not working the night shift for the moment, but I think my decreased stress is also because NICU nursing is a better fit for me. There are so many opportunities within nursing that if a particular job is causing medical or mental health issues, try changing your nursing job!
What’s also relieved some of the new grad anxiety and pressure is recognizing that nursing is a practice. With more time and experience, I can improve my nursing practice. With more exposure to various units or patients, I learn what I like or dislike about specific nursing roles and can set my boundaries and determine my career goals. With more experience, certain medications or typical treatments will become more familiar. I will more easily recognize the signs or symptoms of conditions I regularly encounter. I can determine which skills are essential to master for various units or roles. (Tip: time management is a critical skill, no matter where you work as a nurse)
I have accepted that I’m imperfect and will make mistakes. Even veteran nurses make mistakes. When making mistakes, it’s essential to be transparent to a charge nurse or provider to correct errors or get help and alignment to move forward. Mistakes can serve as lessons. I’ve made mistakes in my engineering and nursing career that I know I will not make again because I never want to feel as compromised or ashamed as when I made the mistakes.
I want to prevent making mistakes that injure or permanently damage patients. One of my NICU preceptors said to accept that I will make mistakes but to spend time making sure I don’t make medication errors. If I spend more time evaluating an unfamiliar medication, dosage, or route, I accept that I will appear slow because of my uncertainty. I will ask for help or clarification. I will move more slowly and risk falling behind on my tasks rather than harmfully administering medication.
ANY new job or career produces increased stress and mental challenges. Some level of discomfort is healthy and helps us to learn and grow. It takes time to learn the protocols or processes of a new organization or unit. No one is perfect, and we all make mistakes. Sometimes, you understand how to be more efficient or effective by making mistakes or witnessing them. It takes time to learn who to ask for help, what requires escalation, and the chain of command. Over time, we know the methods of communication our co-workers, bosses, or patients/clients prefer. Skills cannot improve until you’ve practiced and done them many times. Understanding all this and having the mindset that I’m still learning (“I’m developing, not deficient!“) has helped relieve some of my new grad/novice nurse anxiety.
I hope this post gave some insight into the mental challenges of nursing and the mindset one has to have to thrive as a novice nurse. If you have any advice on how to handle the pressures of nursing or the mental challenges, please share! Thanks for reading! My next posts in this novice nurse series will discuss how I address the physical and emotional challenges of being a nurse.
I went to church Sunday morning with my family and saw the devotional booklet “Our Daily Bread” offered in the vestibule. I hadn’t seen one in a while, but became familiar with them through my mother and relatives from the Philippines, who used them regularly as a daily devotional. The booklet highlights a bible scripture each day and provides a reflection based on that reading. Feeling like I needed to focus more on my spirituality beyond church (it’s so hard sometimes to focus in mass with a rambunctious defiant toddler!), I grabbed one. The bible passage and reflection for that day (April 28, 2019) spoke to me. Because of that, I wanted to share it and invite you to read it at https://odb.org/2019/04/28/gods-retirement-plan/# .
At this moment in your life, what might God be calling you to do for His greater purpose? What new plans has He placed in your path?
Our Daily Bread (April 28, 2019)
The reflection was a great reminder of my second-career journey. Becoming a nurse is the new plan God has placed in my path. I feel I am called to become a nurse to better utilize my talents for His greater purpose. Do you ever feel like you’re on the right path because of the all the “signs” God places before you? You may not have the sign of a burning bush like Moses, but do you feel called to do something, even though you’re uncertain of how exactly you’ll accomplish what you sense you must do? Are you continuously driven towards a vocation without knowing how or if you can really make it happen? And, somehow, a path reveals itself? I feel this way about Nursing – really, I do!
Every step of the way, I feel like God has aligned things for me to allow me to get into Nursing school. If I had waited even one month to look into pre-requisites, I wouldn’t have been able to take the classes I did or complete them before the application cycle. If I had waited one week before researching how to get volunteer clinical experiences, I wouldn’t have become a COPE Health Scholar in a local hospital. If I were in a different volunteer program, I wouldn’t have been able to take patients’ vitals, witness biopsies, circumcisions, C-sections, vaginal deliveries, or perform chest compressions on patients who have coded. God placed people and experiences in my life, to allow me to grow in my compassion, abilities, and skills as a future nurse. Somehow, things aligned or confirmed and re-affirmed my choice to purse a career change. God placed the desire in my heart to consider nursing years ago, but He did not call me into action until now -when I have the social, emotional, and financial support I didn’t have before. His timing was perfect. I prayed to be able to serve God in whichever way He willed, and nursing is where I have now been lead. I have a peace and joy in my heart when I think about my [future] career, but I am still open to God’s vocational plans for me in my life.
Are you called to something new or to continue when you were about to quit? I encourage you to be open to new possibilities or to where God might be calling you. Explore what or where that is, and if you’re called to act, pursue it whole-heartedly. Like Dr. Warwick Rodwell discovering the ancient statue in the Lichfield Cathedral in the “Our Daily Bread” reflection, you could be surprised with the treasure you uncover.