As a bedside nurse, part of my job is to perform patient/family education. It is honestly one of the things I love to do. Since I’m in the NICU, I do most of my teaching to parents and families instead of to my neonatal patients. I can teach parents about how to care for their baby with lessons on feeding, diapering, or bathing, but I can also reinforce their understanding of their child’s diagnosis or medical condition.
At my Level IV NICU, we tend to see a lot of cardiac patients and babies born with congenital heart defects (CHD). Some of these conditions are rare and not easy to understand; even more difficult to understand without knowledge of how a normal heart works. Personally, I never knew or understood blood flow through the heart until I took anatomy and physiology. Not all our parents or caregivers have had anatomy and physiology. So how do I explain what’s going on with their baby?
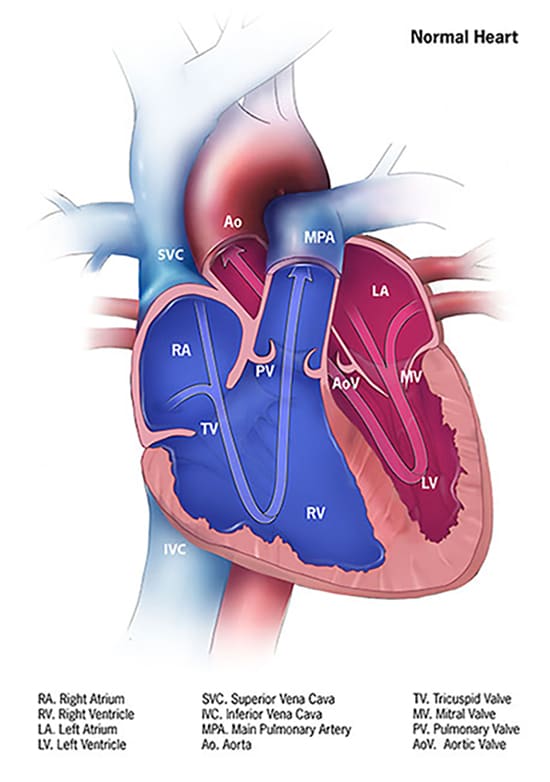
There are reputable websites I can refer to that have pictures to better understand CHD – I think they’re great for healthcare professionals and nursing students as well. One of them is the Centers for Disease Control and Prevention https://www.cdc.gov/ncbddd/heartdefects/index.html.
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
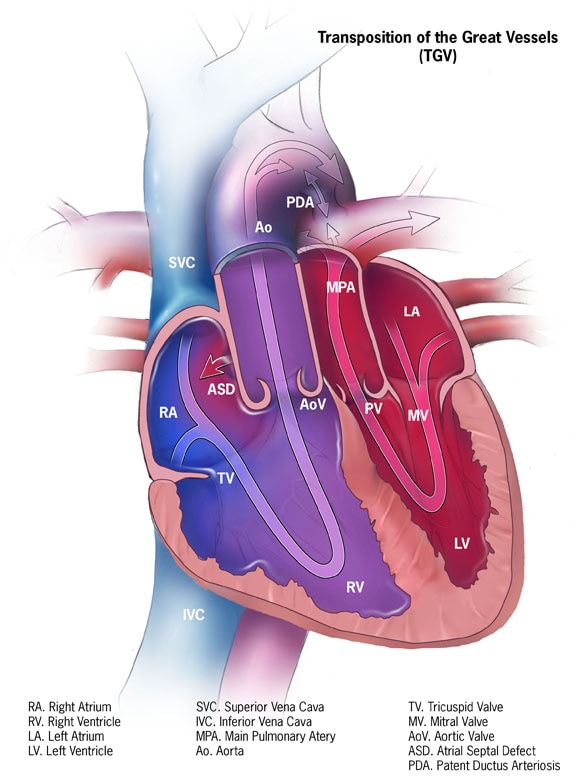
Image from: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities
Another website that’s a great resource for CHDs is Cincinnati Children’s https://www.cincinnatichildrens.org/service/c/cardiothoracic-surgery. Cincinnati Children’s even offers animated heart videos to illustrate various heart conditions. While I love and recommend these resources, I’ve been wondering how I could further simplify patient teaching. In nursing school, I was taught to conduct patient teachings at the 5th grade level. Healthcare professionals should simplify teaching to their patients and patients’ families and use words such that a 5th grader could understand.
Recently, I’ve been thinking about teaching for a family who had a baby come to our hospital with a rare congenital heart defect, Transposition of the Great Arteries (TGA, or d-TGA). They seemed hesitant in explaining their child’s condition. They held up their hands and shared their baby’s arteries need to be like this (as they held their hands up, crossed like an ‘X’) but that their baby’s arteries are like this (as they held their hands parallel) to each other. They were not wrong in their explanation, but I wondered if they understood why it needed to be “crossed”. I felt like a process diagram could have been helpful.
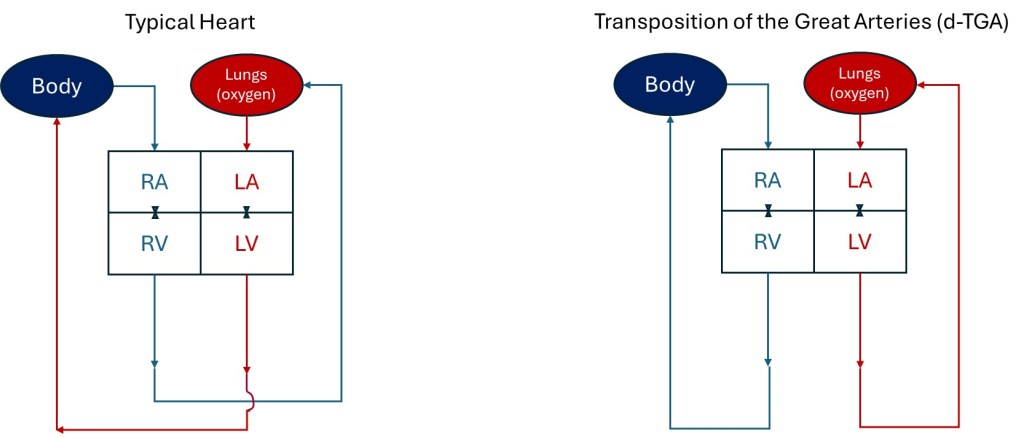
As a former engineer, I used to make flow charts in either designing or explaining existing manufacturing processes. I really wanted to simplify the explanation of blood flow to /from the heart with a process diagram. I drew it out when I got home and then tried to replicate what I drew on the computer. Below are the process flow diagrams I designed, using the same abbreviations as the CDC used to describe parts of the heart in their diagrams: RA = right atrium, LA = left atrium, LV = left ventricle, RV = right ventricle. I also used red to represent oxygenated blood and blue to represent oxygen depleted blood. I represent the tricuspid and mitral valves with the valve graphics used in engineering diagrams. I drew the little curve on the Typical Heart drawing to show the vessels leaving the heart don’t intersect/mix as they cross one another.
Process Flow Diagram representations of the typical heart flow compared to a heart with d-TGA
It’s not an accurate anatomic representation with size and doesn’t depict all the ways the blood enters the heart or how the arteries go up and out of the heart. The vessels and all the valves aren’t even labeled, but I think it easily shows why TGA is such a critical heart defect. From my flow diagram, I think it’s clear the rest of the body can’t receive oxygen with d-TGA because blood from the lungs can’t be delivered to the rest of the body. As a healthcare professional or nursing student, I love the CDC and Cincinnati Children’s images to explain the heart and defects. However, as an engineer, I love the simplicity of my flow diagrams.
If you were a 5th grader, what graphics are easier to understand? What do you think about my depictions? For my next blog post, I’ll share the diagrams I made that show how a baby survives d-TGA until they receive surgery to switch the arteries and correct the flow to the lungs and body. Hint: Look at the ASD and PDA in the CDC graphic for the TGV heart.
Part of my attraction to becoming a nurse was being able to spend more time with my family. Most nurses I knew worked only three days a week, allowing them four free days to do what they wanted each week. I also appreciated that bedside nurses do not take their work home. Most bedside nurses are not on-call or still working when they come home. In my previous engineering career, I worked five days a week and was at work much longer than just eight hours a day. I would sometimes work night shifts and weekends. I was on call frequently or still worked even while home or on vacation. The thought of being free of the tether of work appealed to me as I pursued my career change to become a nurse. Now that I’ve been a bedside nurse for a few years, do I still feel nursing is as family-friendly as I initially thought?
12 hour Shifts
Like most bedside nurses, I am at work 12.5 hours every shift. (Most nurses who work 12-hour shifts are at their place of employment for 12.5 hours due to an unpaid 30-minute meal break). After adding commuting, showering, eating, and sleeping to that schedule, I can do little else on the days (or nights) I work. When I work, I see my daughter for only about an hour each day, regardless if it’s the day or night shift.
When I work days, I must leave the house before my daughter wakes to be at my hospital for a 7a shift. Dayshift ends at 7:30p, and if my commute is nice and short, I get home around 8p. I shower and eat as soon as I come home, but I don’t get to eat dinner with my daughter because it’s too late for her. I have about an hour at home before my daughter’s targeted bedtime at 9p.
When I work nights, I leave the house around 6:15p (since my commute for my new job is shorter now) to start my shift at 7p. My night shift ends at 7:30a, and I get home around 8a. I don’t usually see my daughter when I come home from nightshift because she gets to school before 8a. I shower, eat, and sleep. I target sleeping until 5p. If I get up earlier and my daughter comes home from aftercare before our usual pick-up time, I can spend about an hour with her before I get ready and leave for work.
If I break it down, there isn’t an ideal [12-hour] shift schedule to spend more time with my family on the days/nights I work. Dayshift may be slightly better because I don’t need a sleep/recovery day on my day off as I do after working a night shift. The real advantage of my 12-hour shiftwork is that I don’t have to work as many days each week as in traditional jobs.
Three Shifts Per Week
I can work three 12-hour shifts per week at my current hospital and be considered a full-time employee with benefits. (My prior hospital required a fourth shift one week per month to be considered full-time). Working only three days (or nights) per week means I can have more family time on my four days or nights off that week. The three-shifts-a-week schedule was beneficial for an unplanned trip at the end of March.
Unexpectedly, my husband’s last living grandparent died last month. The funeral service was in Hawaii on a Saturday morning. I hoped to go and support my husband and his family, but I needed to figure out if I could join him since I had just started my new job and had no vacation. My daughter could join him since the trip was during her Spring Break.
Due to my night shift nursing schedule, I joined the family in Hawaii without asking for time off of work. I worked a Thursday night shift – my third shift in a row – and packed as soon as I got home Friday morning. We left that same Friday afternoon and returned home on an overnight flight Wednesday night / Thursday morning. When we returned from Hawaii Thursday morning, I slept and went to work that evening – my first of three in a row. It was a grueling schedule, but I would not have been able to travel with my family for six days without needing time off if I had still worked as an engineer. What other jobs would allow for a personal 6-day trip within 1.5 months of starting?
I was (and still am) on orientation. I did not select my schedule to plan my trip. My supervisors set my schedule to match my preceptor’s. Fortunately, it worked out for me to travel to Hawaii without missing or rescheduling my orientation.
Though it was unplanned and under sad circumstances, my spouse, daughter, and I enjoyed spending time with extended family on our recent trip to Hawaii. I appreciate that my schedule allowed me to travel without taking time off. This pic was taken during on a coastal hike to Makauwahi cave. The hike to Makauwahi cave splits off to a secluded beach. Though my husband and his family had been to the Kauai many times, they had never been to the cave. It was nice to join them in discovering new sites on the island. More importantly, I appreciated being able to celebrate the life of my husband’s maternal grandmother and support him, and be there for family.
I know many other nurses who plan extensive trips on their days between work or by taking only a handful of vacation days. A nurse working three shifts a week could schedule themselves such that they have eight days off between work shifts with no personal time off used. In my previous career as an engineer, I would only have been able to miss work for eight days in a row if I had used vacation days or other forms of leave. The one major caveat to getting desired days off without using vacation or personal time off is nurses still need to get their schedule requests approved or be able to self-schedule. Every nursing job I’ve had allowed me to self-schedule, but I know other nurses who don’t get to select their schedules. My supervisors granted my schedule requests about 98% of the time in my past jobs, so I mostly worked the days/nights I chose (once I was off orientation).
Heavy Workload
When determining if a nurse’s schedule is family-friendly, something else to consider is how much downtime one needs between shifts to recover from work. To schedule a block of days off, as I described above, one usually needs to work a block of days before and after, which can be exhausting. As a night-shifter, I need the day off after work to sleep or nap. My first day off after a block of night shifts is not a day I expect to spend much (awake and alert) time with my family. However, I’ve also had days after working some day shifts where I’ve felt like a zombie. I’ve never felt as drained (emotionally, mentally, and physically) after working as I do as a nurse. I’ve discussed this before in past posts and how sometimes I need a day or two to recover from shift work. Being an engineer could sometimes feel draining, but it was not consistently exhausting compared to being a nurse.
Weekdays Off
Despite needing recovery days, I like having weekdays off as a bedside nurse because it allows me to participate easily in some of my daughter’s school activities. My schedule has allowed me to attend 20-minute in-person parent-teacher conferences in the middle of a weekday afternoon without taking time off from work. I attended my daughter’s award ceremony on a random weekday morning I wasn’t scheduled to work. If my time off coincides with my daughter’s breaks or early dismissals from school, I get to spend time with her exploring our city and going to parks or museums instead of placing her in hard-to-find, expensive camps. I can attend weekday medical or dental appointments for myself or my daughter without taking any time off when I schedule them on days/nights I’m not working.
Weekends & Holidays
While it’s nice to have some weekdays off each week, my schedule requires me to work weekends and a handful of major holidays. I miss spending about half the weekends with my family every month due to work. I have to celebrate Thanksgiving or Christmas early or late if I want to celebrate with family. Some senior nurses at my last job managed to get out of working significant holidays, but no one got out of having work weekends. My current preceptor has worked for over 20 years, but like me, she must work four weekend-shifts each month. Even though I gained some flexibility for weekday activities, I lost spending half my weekends and holidays with family when I switched careers.
Working from Home
Another thing I lost when I became a bedside nurse is the ability to work from home or remotely. I must take time off work if I’m sick, in quarantine, or my daughter is ill (and I stay home with her instead of my husband). I cannot do my job and care for my patients remotely. Remote nursing jobs exist, but not for bedside nurses. On the other hand, being unable to work remotely can be a positive thing for work-life balance because it allows me to separate from work compared to when I was an engineer.
Wait – Let me rethink that. One day in Hawaii, I attended paid mandatory training for my orientation. And if I’m being candid, I spend hours of unpaid time reviewing topics or concepts to prepare for work when I’m not at work. Education and review is my coping mechanism for the stress I face as a novice nurse. Educating myself or doing unpaid training outside of work may persist even as I become more experienced. Nursing requires continuing education. However, I’m genuinely interested in learning about my patient population and ways to provide the best care or be a better nurse. There are always new techniques, equipment, or updated evidence-based practices to learn. I can only sometimes research or learn about new nursing practices during work hours. So there may not be a complete separation from work when I leave the hospital, but it’s an improvement compared to my life as an engineer.
Job & Schedule Variety
I wanted to accurately portray what it’s like to work as a bedside nurse while having a family with this post. However, if a bedside nurse chooses, they do not have to work the traditional three 12-hour shifts per week that I do. Bedside nurses can have one or multiple per diem (one day a week) jobs or work 8 hours a day, five days a week (my last hospital offered 8-hour shifts on the Post-Partum unit). Or, bedside nurses can become travel nurses and work 13-week contracts or whatever they choose to negotiate. There are so many scheduling options out there for nurses. A nurse doesn’t even have to work bedside! A nurse can select a job or schedule that works best for their family and personal life.
The Reality
While nursing can be appealing due to the work schedule, I wanted to review the reality of balancing family and work as a bedside nurse. Despite some drawbacks, my nursing schedule can be family-friendly overall. Is my bedside nursing schedule MORE family-friendly than when I was an engineer? Nope. But I love being a nurse. I love working with my patients and their families and learning, teaching, and helping others. If you are considering nursing as a profession, I hope this blog post gives you a better idea of what a nursing schedule is like and if this profession will allow you to balance work with your family or personal life. Good luck on your journey!
How do you manage stress? Attending school as an older student or pursuing a second career can be stressful. Being a caregiver for aging parents or other family members while working and taking classes can be stressful. Trying to balance parenting and being a nursing or pre-nursing student can be stressful. Do you have a strategy for handling such stress?
My work enrolled me in training last year, where this stress buster wheel was presented and discussed. The stress buster wheel captures evidence-based strategies for toxic stress intervention. The training was for caregivers and healthcare workers to screen and treat patients for Adverse Childhood Experiences (ACEs). However, the stress-buster strategies are an excellent reference for anyone experiencing stress. Do you employ any of these strategies for yourself? Are there ones you’d like to try or implement more?
I like combining several stress busters by going on garden walks or hikes through nature with friends. I connected with a friend (outside of school or class) at least weekly during nursing school to maintain supportive relationships. This helped bring balance into my life, especially when I sometimes felt consumed by my intense 15-month accelerated BSN program. Now that I’ve graduated, I continue this practice to connect with friends regularly.
Across the country, the school year has started for many college students. Students might wonder how to stay organized or manage their time. When I began the journey to become a second-career nurse, I was balancing school, work, parenting, and my personal life. Having a planner was critical for me to manage my time. Below is a list of seven things I included in my planner and recommend students to include in theirs – the last one may surprise you!
Class times. Put in all your scheduled lectures, discussion sections, clinicals, & labs.
Class dates of quizzes, exams, and project due dates. Take the syllabus at the beginning of the semester or quarter and jot down when all the quizzes, exams, practicums, & project deadlines are taking place. Use a different color or shape to identify these in your calendar quickly. I would use blue for quizzes and red for exams or significant projects. The color coding allowed me to easily see when something was coming up and when I needed to study or prepare for something that would impact my grade.
Commute time. I live in Los Angeles, and sometimes commutes can take an hour or more to/from school or work. It’s important to factor this in if commutes can be lengthy in your area, especially if you are responsible for daycare or preschool drop-offs & pickups. Remember to factor in parking as well since that may add to the time it takes to get to a destination. Some people have to park in a garage or lot far from the building where they work, have classes, or have clinical. One of my clinicals took place in a hospital that was a 15-20 minute walk through a tunnel and stairways from the parking lot where we were assigned. If you forget to factor in the extra time it takes to park and walk to your destination, you can end up being late.
Other family members’ schedules. Your family’s schedule is essential. I put in when my parents need me to give them rides to doctor’s appointments or dental procedures. I also add my husband’s business trips (meaning I’m single-parenting my daughter while he travels) or when my daughter has dance, sports, religious education, classmate birthday parties, or school events.
Meals, sleep, & shower/hygiene schedule. If you need 6-8 hours of sleep to function, make sure you schedule it in your calendar. I say this because my targeted bedtimes would sometimes surprise me based on how early I’d need to get up for my commute, etc. Sleep schedules are also important to note if you have children or other family members who require your help to get ready for bed or to get ready for their day.
Study time. The other mom in my nursing program and I found it challenging to study at home once our kids were out of school. I sometimes booked a private room in a library or computer lab to study. Mostly, I would use my spare time to read or do homework between classes or before class if I arrived at school early. I recommend scheduling studying time to realistically determine how much time you have to study, especially if you have other competing obligations such as family or work.
Events or activities that nourish me or bring me joy. I also color-coded these events or activities to quickly glance at my calendar and see that I planned something fun each week. This one activity was not an obligation or part of a busy to-do checklist of duties. It was something I looked forward to doing and had nothing to do with school. I recommend including at least one weekly activity that replenishes you and brings you joy or comfort. Make it happen. The activity could be family game night, happy hour, facetime with a long-distance friend, attending a party, reading a book, yoga, hiking, painting, baking, massage, seeing a musical, or going on a mini-retreat. Each person has different interests and things that bring them joy. Make sure you know what that is for yourself. Ensure you are doing something for yourself at least once a week that helps you reset. You may be a student balancing many things in life, but you’re not a robot. You are a human and have other interests and desires outside of school. Make sure you regularly do things that light you up!
When I had my baby, my husband and I struggled to feed our newborn. I wanted to breastfeed my baby exclusively, but she would not breastfeed well. Influenced by various sources and committed to breastfeeding, I refused to pump or bottle-feed my baby while in the hospital. My baby and I roomed in together while I tried to breastfeed. My husband recalls having to travel with my baby somewhere for light therapy. I vaguely remember this too, but I was tired, delirious from lack of sleep, and recovering from a C-section. I only remember sleeping while my husband and baby were out of the room. In retrospect, my baby most likely went to the NICU because she was jaundiced. She may have been there for only a few hours because I remember waking when my baby and husband returned from wherever they went. Thankfully, the hospital did not admit my baby to the NICU, and we could leave the hospital together. However, our struggles to feed our newborn continued when we got home. Looking back at our experience as new parents, I wish I had known some things about feeding our baby that I know now as an experienced mom and NICU nurse.
Photo by Helena Jankoviu010dovu00e1 Kovu00e1u010dovu00e1 on Pexels.com
Fed is Best
As a NICU nurse, I see term or late pre-term infants (born at 34-37 weeks gestation) who come to our NICU for hypoglycemia (low blood sugar) or hyperbilirubinemia (seen as jaundice/yellowish skin). Often, these term babies come to our unit because they are not eating well. For some babies, parents refuse to feed baby formula while postpartum, and the mom may not have established her breastmilk supply yet. This description reflected us as newborn parents and a likely reason why my baby needed phototherapy.
A build-up of bilirubin in a baby’s body can cause jaundice. Bilirubin is usually processed by the liver and leaves the body as waste. A newborn’s liver may not yet efficiently function, but the baby should be eating/drinking something to produce waste and encourage processing out bilirubin. A newborn baby drinking breastmilk or formula helps curtail jaundice. If a baby is not feeding well or is still jaundiced despite attempted feedings, however, hospitals can treat elevated bilirubin levels (hyperbilirubinemia) through light phototherapy.
Jaundice is normal in newborns, but the hospital monitors bilirubin levels and treats when levels rise above certain thresholds. If the baby’s bilirubin is too high, brain damage can occur. In our hospital, if a postpartum baby needs phototherapy, the baby is admitted to the NICU. Phototherapy in the NICU only happens after multiple attempted feedings and when bilirubin levels exceed treatment thresholds.
Frequent feedings are how parents can reduce bilirubin levels in otherwise healthy babies (and hopefully prevent hyperbilirubinemia that requires NICU care). However, frequent feedings can also help prevent another common condition in our NICU: hypoglycemia, or low blood sugar. If an otherwise healthy baby born to a non-diabetic mom takes enough breastmilk or formula, the baby can usually avoid hypoglycemia. However, if the baby is unable to feed adequately, the baby can develop low blood sugar.
Before a baby goes to the NICU for hypoglycemia treatment and monitoring, the mother and the postpartum staff will attempt to feed the baby. If the mother consents, the baby can be offered formula. If bottle-feeding is still insufficient, a sugar gel is given to the baby orally. The postpartum unit will attempt several feeding and sugar gel administrations before the baby goes to the NICU. If the NICU admits a baby for hypoglycemia, we will place an IV to deliver sugar to the baby as IV fluids. Once the sugar levels in the baby are sufficient, and the baby is drinking adequately, we can reduce the IV fluids and eventually remove IV fluids if the baby can orally consume the needed calories and fluids while maintaining healthy blood sugar and hydration. In the NICU, we try feeding our babies breastmilk if it’s available and not contraindicated (i.e., substance-abusing mother). If breastmilk is unavailable and we need to feed a baby orally, we will give provider-ordered formula to our babies.
For babies admitted for hyperbilirubinemia or hypoglycemia, I sometimes hear the baby barely drank anything because the baby was unable to breastfeed from a mom who wanted only to breastfeed exclusively. Before doctors send the baby to the NICU, the nurses can offer the baby formula if the mom consents or requests it. However, by this time, the baby may have worn themselves out or be too tired to drink from the bottle. It makes me and other NICU nurses wonder, “If the parent or nurses fed the baby from the bottle sooner, would the baby still need to go to the NICU? Is the mother promptly informed of her options if her milk supply hasn’t come in or the baby cannot latch or breastfeed?”
While I’m glad my husband got to go with my baby and accompany her for phototherapy, I would have preferred that my baby not leave my postpartum room at all for treatment or tests. To prevent my daughter from needing to leave our room, I would have pumped sooner to encourage my milk supply and produce milk that my husband or I could bottle-feed my baby. We did not learn until weeks later that my daughter was tongue- and lip-tied, which may have initially made it difficult for her to breastfeed. From my perspective, it’s better to feed a newborn some formula to keep the baby with mom and out of the NICU than to rely solely on breastmilk that may not be available yet or difficult for the baby to access.
Pumping is Okay
I was offered to pump in the hospital but refused, thinking I would breastfeed. My doula recommended not to pump until after the first month, so I tried holding off on pumping in an attempt to have my baby latch, help establish our breastfeeding rhythm, and set my breastmilk supply.
I didn’t want to feed her from a bottle because I didn’t want to cause nipple confusion and have my baby prefer the bottle over breastfeeding. When we got home, I thought I was doing okay breastfeeding, but when we brought our baby to her 1-week checkup, she wasn’t gaining enough weight. We brought her to her 2-week checkup, and her pediatrician still didn’t think she was gaining enough. My daughter fell in the 2nd percentile on the growth chart. (I did not discover until months later that my husband and his siblings were so small as newborns they were not even on the growth chart). We were strongly encouraged to start bottle feeding her formula.
Wrought with guilt, we decided to feed her some formula, and I began to pump. By this time, I had developed mastitis (Mastitis is a painful infection in the breast caused by bacteria introduced by breastfeeding. It also caused me to have body aches, a high fever, and chills. Imagine dealing with this while trying to care for a newborn!) My supply was woefully insufficient, and most of my daughter’s caloric intake was formula once I started to pump while battling mastitis.
Formula is Okay
It is okay to use formula if you are not producing breast milk or enough breast milk/colostrum to feed your baby. I wanted to exclusively breastfeed because I learned about the benefits of breastfeeding and how it’s the best, natural, and easiest way to feed my baby. It’s great for baby bonding and helps provide passive immunity to the baby. However, I got mastitis TWICE within the first month or so of my daughter’s life. We also learned my daughter was tongue-tied, making it difficult for my daughter to breastfeed. Not until later did I meet other mothers who breastfed AND bottle-fed their babies or moms who exclusively pumped. (Moms who exclusively pump only feed their babies breastmilk from a bottle). Had I not been so attached to exclusively breastfeeding, I could have adapted and explored these other options earlier as a new parent.
Do What’s Best for You and Your Family
Aside from taking antibiotics, the way to clear a mastitis infection from the breast is by breastfeeding or pumping. My daughter preferred the bottle by this time, so I relied on pumping to clear my infection. Pumping (and antibiotics) eventually relieved the pain and released the mastitis in my breasts, but the repeated infections impacted my supply. Encouraged by my doula, I remember three days where I spent about 9 hours pumping (diligently pumping 45 minutes every 2 hours, per her recommendation) only to produce about 1 ounce of breastmilk daily. I was so exhausted and upset by the results of my efforts. I also felt cut off from my daughter while I pumped (Because I couldn’t figure out how to safely hold her with all the pumping tubes hanging from my body, my husband or parents would take her while I pumped). After the three days dedicated to pumping round-the-clock, I decided it was not worth it to continue to pump. It was more important for me to be with my baby than to try giving her my pumped breastmilk.
I still held out hope for breastfeeding. Once my infection cleared, I tried to breastfeed my daughter using an SNS (supplemental nursing system – a tube placed on the breast but connected to a bottle to measure and ensure the baby has adequate intake). She was already used to the bottle nipple and did not take to the SNS. I attempted multiple times, but she would refuse to feed through the SNS, and I would end up with formula spilling all over my chest.
I share a bit of my breastfeeding journey to emphasize that there are many ways to feed and nourish a baby. In the end, so long as the baby is healthy and safe, parents decide what works best for them and their family. The caregivers’ mental health and well-being are as important as the baby’s. The way you choose to care for your baby may not resemble how other families do things, and that’s okay. I was ashamed for not breastfeeding my daughter for as long and in the way I hoped, but I felt my attachment to breastfeeding distanced my baby from me and caused so much anxiety and distress. Parents should not be ashamed of doing what is best for them and their families.
In the NICU, I meet moms who feel nervous they cannot directly breastfeed, yet they can pump and produce enough breastmilk to meet their baby’s needs. I meet parents who are ashamed they don’t have a separate nursery for their baby. We live in Los Angeles – not every family can afford to pay for a home with different bedrooms for each of their children! Many of our parents rely on WIC because they can’t afford to purchase formula. Getting formula from WIC is better than diluting formula or not feeding the baby enough nutritious calories. I try to assure the parents I see they can do what works for their family – it doesn’t need to match other families.
I felt defeated when I finally gave up pumping and breastfeeding. I wish I gave myself a little grace as a newborn mom and wasn’t so hard on myself. I felt so much grief over my inability to mother and feed my child as I thought I should that it made me feel inadequate as a mom. I was separated from my baby while I pumped, trying to salvage any breastmilk I had. I cried every day when I was pumping or trying to breastfeed. Ultimately, I fed my baby adequately, thanks to formula, and my child is now a healthy school-age girl. She still falls on the low end of the growth chart, but her father and I are not tall, so my daughter’s standard is the tenth percentile or less.
As I reflect on my experience as a new mom, I hope to impart grace and support to other new parents now that I’m a NICU nurse. If a caregiver is feeding their baby adequately, caring for and bonding with them, and keeping them safe, I want them to know they are doing a great job! I also want them to know it’s okay to make adjustments as needed or change their minds about how they want to do things. Parents can adapt their plans according to the family’s needs.
I originally wrote this post to give insight on how to lower the likelihood of hyperbilirubinemia or hypoglycemia (and admission to the NICU) through frequent feedings. If this information helps reduce NICU admissions and prolong in-room bonding between caregiver and baby, I would be ecstatic. Ultimately, I hope this post reassures parents (and serves as a reminder to myself) that there are many ways to care for a baby. There are no perfect parents; there are no perfect children. We’re just doing our best with the information and resources we have. Good luck to you on your journey!
They say when you begin a journey (or a big project) to start with the end in mind. Before I even switched careers, I did an online job search for the job I wanted. This preliminary job search helped direct and guide what I did to prepare me for my career change.
Do this before you pursue a bunch of training and education for a career change. Look at what your dream job requires. An old co-worker of mine became a nurse while she was working full-time and tried to apply to her dream job with a government organization. Unfortunately, she wasn’t qualified because her program was not accredited. She shared how her entire motivation to become a nurse was to work for this employer, and how devastating it was to discover that she couldn’t even apply to the organization.
To be honest, I *still* search for other jobs to this day to motivate me in getting the training, certifications, or experience I need for my next possible position.
If you are a career switcher, what advice do you have for people considering changing careers? Share in the comments below!
It’s the time of year when many students are getting acceptance letters to nursing schools, and I’ve seen posts on discussion boards asking for advice on choosing a nursing school. Since I lived in an area where there were many Nursing school options, I had to filter through and determine which programs were the best fit for my family and me. In this post, I offer advice on what to consider when choosing nursing schools and insight into how I chose my nursing program.
Accreditation & BRN Approval
First and foremost, ensure the programs you are applying to are accredited and approved by the Board of Registered Nursing. In the US, you can visit your state’s Board of Nursing “Education” section to search the list of approved nursing programs. The BRN divides the list of programs by pre-licensure programs (LPN, ADN, BSN, and entry-level Master’s of Nursing program) and advanced practice programs. If you’re even wondering which schools offer nursing programs, the BRN list is an excellent overview of approved programs in your state.
You do not want to spend tuition and time at an institution that the BRN hasn’t approved because you won’t be able to sit for your licensure exam (NCLEX). The BRN will list programs with full and conditional approvals. Consider how a conditional approval may affect you if, for some reason, the BRN removes their program approval before you graduate. Can you ask the school or program why they received conditional approval and what they are doing to ensure full approval? I shied away from newer programs and didn’t apply to conditionally approved ones. I sought only fully approved and established programs because I didn’t want to take my chances with enrolling in a conditionally approved program or a program that could easily dissolve.
NCLEX Pass Rates
While visiting your state’s Board of Registered Nursing website, search for NCLEX pass rates (For California, where I obtained my degree and license, the website is https://www.rn.ca.gov/education/passrates.shtml). The pass rates provide a sense if the program you’re applying to adequately prepares its students for the NCLEX, the exam required to earn a registered nurse license.
Graduation Rates
Consider on-time graduation rates for your potential schools/programs. Per the amended Higher Education Act (HEA) of 1965, colleges must publish information regarding graduation rates, retention rates, and student diversity.1 Due to the National Center for Education Statistics (NCES) definitions, graduation rates for people with second degrees or who have already attended other postsecondary schools aren’t necessarily part of a school’s published on-time graduation rates.2 However, whether you are pursuing Nursing as a second or first degree, I think graduation rates are something to consider and request from your potential school or nursing program. If your nursing program does not readily share graduation rates, you can also view graduation rates at the following NCES website: https://nces.ed.gov/collegenavigator/.
Graduation rates are essential to consider to manage your expectations. If you’re choosing a nursing program because it’s shorter than others, but their on-time graduation rate is 50% or less, you run a 50% or greater chance of spending more money and extending the amount of time to earn your degree to get your nursing license. There is a private, for-profit university known for not having a waitlist for their nursing program here in Southern California, so many students apply and attend. They can start nursing school quickly instead of getting waitlisted or possibly rejected from other less expensive, competitive programs. The program is over $100,000 for the projected three years it takes to get a BSN from this for-profit, private university. The three years are appealing over traditional four-year bachelor programs despite the cost. However, the for-profit university’s on-time graduation rate is as low as 38% for their Los Angeles campus. When talking to nursing alumni from this university, many agree that it’s easy to get held back a semester and that the program can take longer than expected. However, the additional cost and time are worth it for program graduates because it was an avenue to get their nursing degree when other options were limited.
I’m not saying to shun schools with low graduation rates. Consider graduation rates, so you know what to expect. It’s better to be aware of potential costs up-front than to be surprised when you need to spend more time and money than what the program advertised.
Tuition
An obvious consideration when applying to schools is tuition. How much of a student loan will you need to attend school, or can you avoid taking a loan? For what kinds of financial aid are you eligible? (Second-degree holders do not qualify for pell grants). Can you afford private schools? Public schools are far more affordable but can also be more competitive.
Do you have grades, work, or volunteer experience that make you a competitive candidate? Do you need to repeat pre-requisite courses to increase your GPA and become a more desirable applicant? The extra time to repeat pre-requisites might be worth it if it saves you tens of thousands of dollars in tuition fees. (CAUTION: Be careful with re-taking courses or exams because some schools only accept a certain amount of repeats or will only accept a repeated course or entrance exam like the TEAS if it’s after or within a specific timeframe).
Program Length
The duration of the program is an important consideration. If you’re not working while going to school, that extra time in school is potential income lost. It is ACTUAL income lost for people with a prior career like me. Like most people looking to switch careers, I wanted an accelerated program to work as quickly as possible in my newly chosen profession. I didn’t want to be in school for four years to switch careers. Since I already had a bachelor’s degree, I was eligible to apply to accelerated Bachelor’s of Science in Nursing (ABSN) programs. In my area, these ABSN programs range from 12-24 months.
Location
Consider the location of your nursing school. Are the programs to which you’re applying local? Will you need to spend an hour or more commuting to school? Some of my classmates moved from one part of Los Angeles to another part of Los Angeles to avoid traffic that would add to their commute. Can you carpool with someone to allow you to take the carpool lanes and make your commute more bearable? Other cohort mates moved across the country to attend our ABSN program. All the nursing schools I applied to were within a reasonable drive from my home.
The school I chose happened to be the farthest from my house. When I started nursing school, I was lucky enough to discover one of my cohort-mates lived in my neighborhood, so we agreed to carpool. She became one of my best friends, and we used the carpool time to study and quiz each other (or vent about our lives as the only moms in the program).
Clinicals
If you can, try to find out where the schools do their clinicals. You can ask the program staff or alumni. Doing clinicals at hospitals or areas you wish to work offers excellent exposure to potential employers. The pandemic limited clinical rotations, so the recent years’ clinicals may not represent what is typically provided in a nursing program. However, you know a program is decent if they were able to send their students to good clinical locations amidst a pandemic. Also, keep in mind the places of clinicals may add time to your usual commute to school, and some may occur during the evening or night shift. Knowing this information upfront helps manage expectations.
Impressions of Alumni & Working Nurses
Talk to alumni about the programs you’re considering. Some questions you could ask:
Do they recommend going there?
Did alumni feel adequately prepared by their program?
How long did it take to graduate?
How much did it cost them vs. the advertised tuition?
What attracted them to their program?
What do they feel were the pros and cons of their program?
Talk to working nurses you trust and respect. How is working with new grads from particular schools or programs? Do some nurses seem better prepared than others? What are working nurses’ impressions of students from that school/program when they do clinicals? Do they have program recommendations? Would they recommend their alma mater?
As I shared in a prior post, I networked with others before I applied to ABSN programs and before I accepted the offer to attend my school. Talking to others about the various schools assured me that the schools I applied to were a good fit for me. My top choice school would change from time to time, but all schools I applied to were great options for my family and me.
My Choices
After working hard to make sure I’d be a competitive nursing school applicant and getting straight A’s on all my pre-requisites, I got accepted into three ABSN programs lasting 12 months, 15 months, and 24 months. The cheapest program was the 15-month program from a public university, while the 12-month program at a private university was more than twice the cost of the 15-month program and the most expensive, by far. The 24-month program tuition was slightly higher than the 15-month program but had the longest duration. I chose the 15-month program to save money and time and figured the additional three months it would take to earn my degree over the 12-month program would be worth my sanity. Additionally, the 12-month program had much lower NCLEX pass rates, making my choice even more straightforward.
Although this post was prompted by someone considering nursing school offers, ideally, all the above considerations would be made BEFORE applying to nursing programs. Whether you’re sifting through nursing school offers or selecting which schools to send applications to, I hope this post helped. Please share in the comments below if you have other considerations or advice to contribute when selecting a nursing program. Thank you for reading, and good luck on your journey!
——-
Footnotes:
Per the National Center for Education Statistics, “The overall graduation rate is also known as the “Student Right to Know” or IPEDS graduation rate. It tracks the progress of students who began their studies as full-time, first-time degree- or certificate-seeking students to see if they completed a degree or received a certificate within 150% of “normal time” for completing the program.”
The National Center for Education Statistics (NCES) notes that “students who have already attended another postsecondary institution, or who began their studies on a part-time basis, are not tracked for this rate.”
As a follow-up to my blog post last week, I thought I’d share some general tips and questions to consider when networking with others if you’re interested in switching careers. Scroll through the slides below for my tips!
Do you have any additional tips for networking or questions to ask others when considering a career change? Drop a comment below if you have something to share that you found helpful for you!
A friend recently asked me how I switched careers as a working mom. She was considering switching careers, so she wanted to know about some of my steps before becoming a nurse after years of working as an engineer. Some advice I gave her:
Talk to others in your profession of interest.
Ask them about their experience, challenges with their work, how they like their jobs, and their favorite part of their work.
Inquire about the education or training they completed to get where they are and how they got their job.
Before entering nursing school, I did these things to get an idea of what nursing was like and what I needed to do to become a nurse. To put it simply, I networked.
Build on your connections: Talk to Others You Know.
I talked to all the nurses and people in healthcare I knew. I had a couple of cousins who were nurses. Aside from periodically picking their brains at family gatherings, I asked if we could meet for lunch to discuss nursing. I asked them what they liked and disliked about nursing. I learned how they chose and got accepted to their nursing school and how long it took them to complete their programs. They shared how expensive their tuition was. I asked their impression of the various programs and the graduates their hospitals tend to hire.
If I had any nurse acquaintances, I tried interviewing them, too. I reached out to nurses I met from my mom’s club and nurses I knew from church. I offered to have coffee with them to discuss nursing. I had an old friend from college who had a friend that went through an ABSN program, and I asked my friend if I could reach out to her. My friend put us in touch, and I was able to ask her questions about her accelerated nursing program. I reached out to EVERYONE I knew who could give me some perspective on the nursing profession or nursing school.
Form Connections: Talk to Others You Don’t Know.
I even reached out to nurses I didn’t know at all. I joined a MeetUp for nurses. I explained my interest in nursing and my desire to meet more working nurses. When I’d go to my personal doctor’s appointments, I’d talk to MA’s, phlebotomists, and nurses and ask them how they like their job, what training they went through, and if they had advice for aspiring nurses. I even reached out to a nurse in my neighborhood’s Facebook Buy Nothing group. She graduated from a nursing program to which I was applying. I eventually became friends with her and was able to request her to review one of my nursing school application essays. (Sidenote: When I experienced my first death after a code blue, my nurse friend from church recommended I view a TED Talk given by a nurse about grief. The TED talk speaker turned out to be my neighbor/friend from my Buy Nothing group!)
Strengthen Your Connections: Continue to Network.
All nurses and even non-nurses I approached to discuss healthcare and nursing were supportive of me. All were willing to answer my questions. As I started to meet more nurses or people in healthcare, I felt I was getting a more accurate picture of Nursing.
I first heard the brutal truth about nurse burnout during my second Nurse MeetUp event. The host of the MeetUp, Cara Lunsford, didn’t want to scare or discourage me, but she also wanted to acknowledge the challenges nurses face and support working nurses. Until that meetup, I didn’t realize the nursing shortage wasn’t just that not enough people were entering nursing school. Cara shared that a lack of nurses also exists because many nurses leave the profession. The MeetUp was a nurses’ week event, and Cara’s company, Holliblu, hosted a free screening of the 2014 documentary, “The American Nurse.” I thought it was excellent exposure to various facets of nursing and the potential challenges I would face as a nurse. Since then, now that the world has experienced the COVID pandemic, I think more people are aware of nurses’ working conditions and burnout. My continuation to network emphasized that it’s good to learn as much as you can about your area of interest – the good, the bad, the ugly – before deciding whether or not it’s for you.
Join Professional Organizations or Online Groups
After meeting with my nurse friend from church, she suggested I join a professional nursing organization’s Facebook group. She was part of a local chapter of the American Association of Critical-Care Nurses (AACN). I asked to be part of the Facebook group before I was even in nursing school. Because I was part of the Facebook group, I learned about and attended a sponsored event with AACN during nursing school, even though I wasn’t an official AACN member. I spoke with critical care nurses who provided unsolicited but valuable advice on where NOT to work after graduating from nursing school. Eventually, I became a paid member of AACN as a nursing student. (Hint: Membership fees are cheaper if you join professional organizations while still a student. Also, professional memberships are good to put on your resume as you apply to new grad jobs.)
Volunteer
Before I became a nurse, I tried immersing myself in the working environment of a nurse. I reached out to a former co-worker and fellow engineer who volunteered at a hospital before she joined a full-time MBA/MPH program. Her volunteer program, COPE Health Scholars, seemed rigorous and offered excellent training. It was more than simply pushing patients in their wheelchairs or bringing them water. Volunteers took vitals, assisted CNAs with patient activities of daily living, and participated in codes, as allowed by their certifications. I learned about the program through her, and I applied. I passed the rigorous application process and training and got accepted into the COPE Health Scholars program while working as an engineer. I volunteered throughout my pre-requisites, nursing school applications, and until my ABSN program started. I met many more nurses and worked with patients in various units. The program further cemented my desire to become a nurse, gave me valuable clinical experience, and helped with my nursing school applications. Perhaps even more beneficial for a handful of other volunteers, the program helped them recognize that healthcare was not for them.
Return the Favor: Give Back
Seize networking opportunities, but don’t be an opportunist. When networking, it’s not just about what you can take from others. If you want to build relationships and good faith, offer something in return. Share your wealth with others. Your wealth is not just monetary wealth – you have skills, time, knowledge, experience, connections, and resources. Some examples of how I tried to reciprocate with others I networked with:
I offered to buy lunch or coffee for nurses who agreed to meet with me.
When my entrepreneurial MeetUp host inquired about corporate sponsorship or contacts, I gave as much insight as possible about the company that employed me as an engineer. Even though my work experience was in the consumer products sector, my former employer led a campaign to support nurses and the nursing profession.
I signed up to volunteer at AACN community service events and got some of my nursing school classmates to join me. (AACN eventually canceled these Spring 2020 community service opportunities due to the pandemic).
When another mom’s club member approached me to explore nursing as a career change, I readily met with her during a study break.
I put my friend, who is exploring a career change, in touch with the one person I knew who worked in her field of interest.
I have to admit I always found the term “networking” intimidating, but it’s something I had done before changing careers without realizing it. I hope what I’ve written provides examples of how you can network – or connect with others – to explore a second career. I’d love to hear about ways you network, what’s worked/didn’t work, and what you thought was helpful! Good luck on your journey!